Last week, the New Mexico Republican Party called on the state's governor to ease lockdown restrictions and slowly reopen businesses despite the continued spread of coronavirus. According to KUNM, a group that say's it's backed by the state GOP is now calling for businesses to defy lockdown orders and open anyway, but they aren't getting the response they hoped for.
This Monday, the group "Take Back New Mexico" organized a Facebook event that called for non-essential businesses to reopen in a show of defiance against lockdown orders. O’Rion Perry, one of the event's organizers, says the state GOP produced the online recruitment form for businesses that wanted to participate. While the list was never posted, Perry said he wanted the businesses to announce their participation themselves. But none of the 75 or so mostly rural businesses that Perry said had signed on had announced anything by Tuesday. According to Perry, they’re afraid of the legal consequences of violating lockdown orders.
When asked by KUNM about their alleged participation in the event, the New Mexico GOP released a statement saying that while the health and safety of all New Mexicans come first, they believe "the governor’s decision to keep big box stores open and close locally-owned mom and pop businesses across the state is wrong."
"We can responsibly have social distancing at all establishments, something that’s NOT happening at the national chains," the statement read. "Meantime, our local businesses are collapsing, closing and people may never recover. We encourage local governments to breathe life back into their communities and support responsible resolutions and calls to state government to reopen businesses."
According to the Daily Lobo, about 16 carfuls of people showed up outside the State Capitol for "Operation Gridlock." Among the participants was Alexis Martinez Johnson, a Republican running for Congress in New Mexico's 3rd Congressional District.
Diane Roberts, a professor of English at Florida State University, has written a brutal rebuke of her state's Trump-loving governor and his reluctance to take the COVID-19 pandemic seriously.
In a Washington Post editorial headlined "In Florida, we love our beaches. Thanks to our governor, now we can die for them," Roberts eviscerates Gov. Ron DeSantis for encouraging cities and towns to reopen beaches during a time when the number of COVID-19 cases is still spiking in Florida.
"DeSantis has dithered, obfuscated and delayed," she writes. "He wouldn’t tell Floridians to stay home until he got the go-ahead from Trump; like Trump, he shills hydroxychloroquine as a supposed coronavirus miracle cure. He wants to reopen Florida’s economy sooner rather than later and has assembled a dubious task force full of CEOs and friendly politicians, but no doctors, no scientists."
She also slammed DeSantis for deferring to business interests in keeping large parts of the economy open, including his infamous designation of professional wrestling as an "essential" business.
"But hey, at least we can watch Ronda Rousey wrestle Charlotte Flair or the Street Profits tag team take on the Viking Raiders," she concludes. "We can pretend that everything’s all right, that the Magic Kingdom will always be there, that Wet Willies will keep slinging daiquiris and that Florida will never impose too much reality on us. We can, after all, still go to the beach."
On March 17, Medicare chief Seema Verma stepped to the podium at a White House coronavirus briefingand unveiled a “historic action” to promote virtual medical care, or telehealth.Verma temporarily lifted a variety of federal restrictions on the use of the service, which had been limited to rural areas. She praised telehealth, saying it could handle routine care for an older patient with diabetes without risking a visit to a medical office. She said a Medicare recipient with mild flu-like symptoms could receive advice from a doctor at home “instead of leaving the house and sitting in a waiting ...
Scammers always look for new opportunities to steal money from unsuspecting victims, and the coronaviruscrisis is no different.As Americans wait anxiously for their stimulus paymentsto arrive, a federal government watchdog group warned taxpayers that scammers will come after those payments.The Treasury Inspector General for Tax Administration (TIGTA)said it anticipates “criminals will engage in various scams and schemes in attempts to intercept Economic Impact Payments, and/or steal sensitive taxpayer information during these challenging times.”It said the IRS will not call, text or email you ...
In the business world, supporters of stay-at-home orders and aggressive social distancing have been arguing that ending them prematurely — and causing unnecessary deaths from coronavirus — will ultimately hurt the U.S. economy a lot more than the financial pain that is presently being felt. But one person who doesn’t see it that way is billionaire shipping magnate Liz Uihlein, a major GOP donor and an economic adviser to President Donald Trump. And Bloomberg News reporters Anders Melin and Polly Mosendz, in an April 21 article, describe some of the actions Uihlein is taking politically to discourage social distancing and stay-at-home orders.
Uihlein, Melin and Mosendz report, is supporting a petition to recall Democratic Wisconsin Gov. Tony Evers for his stay-at-home order.
“As protests grip Wisconsin and other states with Democratic governors, the debate is dividing neighbors, politicians and business executives,” the Bloomberg journalists notes. “Big company CEOs — Democrats and Republicans alike — have generally urged caution about reopening because of the health risk, yet some of the GOP’s biggest donors have been pushing hardest on the side of lifting restriction.”
Melin and Mosendz observed that although Koch Industries Chairman Charles Koch has “questioned blanket shutdowns…. few have objected more strongly than Liz Uihlein, chief executive officer of closely held Uline.”
Uihlein has a history of downplaying the severity of COVID-19. In a March 13 e-mail to Illinois politicians, the Uline CEO asserted, “The media is overblowing COVID-19. At what point do we go back to our normal lives? This has been a huge disruption.”
But the pandemic that Uihlein believes the media are “overblowing,” according to researchers at John Hopkins University in Baltimore, has killed at least 178,845 people worldwide (as of early Wednesday morning, April 22). And that includes over 45,000 deaths in the United States, which has become the coronavirus epicenter of the world.
Uihlein has been criticized for not doing enough to encourage Uline employees to work from home. Melin and Mosendz note that Uline is offering an extra $5 per hour to employees who work on site rather than working from home.
Some restaurants in Georgia are refusing to open their doors to customers even though Gov. Brian Kemp (R) is lifting his stay-at-home order earlier than most states.
“It’s insane," Buttermilk Kitchen owner Suzanne Vizethann told the paper. "It’s almost just as stressful as when we got the news of the (dine-in) closure."
“We feel like we just got in a good rhythm. We’ve got a system. We turned the living room and dining room into a fulfillment center," she added. “We simply do not feel safe, nor are we ready to open back up in days of getting the news."
Restaurant operator Hugh Acheson insisted that he would not open until "I weigh science and risk and have the confidence that I can do this correctly and safely for my employees and the people I serve."
Brian Maloof of Manuel’s Tavern said that opening his restaurant is "simply not happening."
"Being closed has not been fun but it’s been the safest, best thing we could do for our staff and customers," Maloof wrote on Facebook.
Others pointed out that additional guidance was needed from the governor.
“Until we have that, we don’t know,” Gianni Betti of Cibo e Beve explained to the paper. “We need to know if a server has to wear gloves, masks. We need more information.”
As protests pop up around the country calling for the end to state lockdown orders even as the coronavirus rages, the ideological agendas behind these protests are being exposed, as many of the demonstrations have been found to be orchestrated by various right-wing groups. But another fringe movement has found a home at the demonstrations, namely the nation's anti-vaccine activists, who find common cause with the protesters, many of whom have expressed anti-vaccine sentiments online and on their banners.
According to The Daily Beast, the addition of the anti-vaccine movement to the lockdown protests makes health agencies' work ahead even more complicated.
"Health officials have said that a vaccine for coronavirus is one of, if not the, surest ways to emerge through the crisis and return to a semblance of social normalcy," writes the Beast's Will Sommer. "But that depends on wide-scale cultural acceptance of the vaccination—which optimistically could be 18 months away from production—and the coronavirus pandemic has drawn more online interest to anti-vaccine causes."
According to University of Colorado Denver sociologist Jennifer Reich, much of the rhetoric emanating from lockdown protests echoes the rhetoric of anti-vaccine activists. Reich’s research has found that the rise in unvaccinated children has been the result of two trends: pressure on parents to research every detail of the choices available to their children; and the idea that individuals themselves are better equipped to handle their own health choices.
As anti-vaccine parents anticipate a coronavirus vaccine and claim they can best handle the decision to vaccinate their children, the lockdown protesters have declared themselves the best judges as to whether or not they can go out in public and risk infecting themselves or others, and it's a dangerous combination.
President Donald Trump tweeted Wednesday morning that he has instructed the U.S. Navy to "shoot down and destroy" any Iranian vessels that "harass" American warships in the Persian Gulf.
Critics slammed the threat as an effort to distract from the president's abysmal response to the deadly coronavirus pandemic, which has now infected more than 800,000 people and killed at least 40,000 in the United States.
"If the xenophobia isn't doing the trick and providing a good enough distraction, there's always the classic authoritarian move: gin up a war," said Matt Duss, foreign policy adviser to Sen. Bernie Sanders (I-Vt.).
Trump's tweet came a week after the U.S. Navy accused Iranian gunboats of making "dangerous and harassing approaches" to American warships in the Persian Gulf.
"I have instructed the United States Navy to shoot down and destroy any and all Iranian gunboats if they harass our ships at sea," Trump wrote.
"The mother of all distractions," Trita Parsi, executive vice president at the Quincy Institute for Responsible Statecraft, said of Trump's tweet.
The president's threat closely followed a "Fox & Friends" segment on the Islamic Revolutionary Guard Corps' successful launch of a new military satellite on Wednesday.
John Bolton, the ultra-hawkish former national security adviser who has pressed for war with Iran for years, tweeted that "Iran's launch of a military satellite is proof we are still not applying enough pressure, deterrence has not been restored, and coronavirus is not slowing down the ayatollahs."
President Donald Trump has been pushing for governors across the United States to reopen their economies amid the COVID-19 pandemic that so far has killed tens of thousands of Americans.
However, a 2014 tweet that Trump wrote about a small outbreak of the Ebola virus in the United States is coming back to haunt him.
The tweet in question slammed American governors for lifting their Ebola-related quarantines, which is exactly the same policy that Trump is now pushing for governors to enact in the midst of a far deadlier outbreak of disease.
"All the governors are already backing off of the Ebola quarantines," Trump wrote at the time. "Bad decision that will lead to more mayhem."
COVID-19 has already killed an estimated 45,000 Americans over the span of just six weeks, while the Centers for Disease Control says that a grand total of two Americans died from the Ebola virus in 2014.
For the past few weeks, television doctor Mehmet Oz has been going on Fox News to aggressively promote treating people infected with COVID-19 with hydroxychloroquine, an anti-malarial drug that was singled out by President Donald Trump during his press briefings.
During an appearance on "Fox & Friends" Wednesday, however, Oz backed off his promotion of the drug and suggested more testing was needed to conclude whether it was effective in treating COVID-19.
"The fact of the matter is, we don't know," Oz said. "Thankfully, these medications are prescription only, so doctors are desperately awaiting the completion of the higher-quality randomized trials... we are better off waiting for the randomized trials Dr. Fauci has been asking for."
CNN's Oliver Darcy reports that Fox News in recent days has "all but stopped" mentioning hydroxychloroquine after promoting it as a treatment literally hundreds of times over the last month.
"The quite abandonment of hydroxychloroquine comes as studies indicate it is not an effective treatment against the coronavirus," Darcy reports. "A French study found last week that the drug does not help patients with the virus. And on Tuesday, a study of hundreds of patents at US Veterans Health Administration medical centers found that patients who took hydroxychloroquine were no less likely to need ventilation and had higher death rates than those who didn't take the drug."
Amid the stress and confusion of coronavirus shutdowns and social distancing orders, it can seem to older patients as though everything is on pause. Clinics have postponed regular office visits. Patients worry about going to pharmacies and grocery stores. There’s even anecdotal evidence that people with serious issues such as chest pain are avoiding emergency rooms.
One important fact must not get overlooked amid this pandemic: Chronic health conditions still need attention.
If you had diabetes before the pandemic, you still have diabetes and should be monitoring your blood sugar levels. If you were advised to follow a low-salt diet before the pandemic to control your blood pressure, you still need to follow a low-salt diet during what my spouse calls “the duration.” If you had to check in with your doctor if your weight increased from underlying congestive heart failure, you still need to check your weight daily and call your doctor.
As I remind my geriatric patients, taking care of chronic conditions is even more critical right now as the new coronavirus raises the risk for people with underlying medical problems.
Lungs, heart and even kidneys
If you have chronic medical conditions and you become infected with the coronavirus, you’ll likely face an increased risk of developing severe symptoms.
The Centers for Disease Control and Prevention looked at a sample of U.S. patients with COVID-19 and found that
COVID-19 primarily affects the lungs, and people with lung diseases, such as COPD, have less “pulmonary reserve,” which is like having a backup generator waiting to kick in if the power goes out. So, what might have been a mild infection for someone else can develop into a severe infection for someone with lung problems.
Beyond the lungs, doctors and scientists are starting to see signs that COVID-19 may have devastating effects on the kidneys and heart. An extreme immune system response known as a cytokine storm can damage organs, and mini blood clots have developed in some patients.
High blood pressure, congestive heart failure or diabetes can also increase the risk of developing severe symptoms from COVID-19. In the CDC sample, 73% of older patients hospitalized with COVID-19 also had hypertension, about a third had diabetes and just over half had cardiovascular disease.
How to keep seeing your doctor
Managing chronic conditions amid a pandemic is not easy. It requires adjusting daily routines and dealing with new obstacles.
One of the challenges is medical appointments. During the pandemic, most geriatric clinics have postponed in-person visits for routine check-ups to avoid exposing patients or staff to the coronavirus. But that doesn’t mean your doctor isn’t there for you.
My clinic, for example, has transitioned most patient appointments to telehealth. This allows us to keep in touch with our patients and their symptoms and to adjust treatment plans in real time.
Online portals with “virtual waiting rooms” allow for video visits between patient and doctor. For patients who don’t have access to the internet or aren’t as comfortable with the technology, the telephone works, too. Patients can send photos of injuries. Over 90% of my clinic visits with my geriatric patients are now by telephone. We schedule time for the clinic appointment, the clinic staff registers the patient, and then I call the patient for the check-up.
I was in the middle of one of these visits recently when a patient asked me if I thought they should try telehealth. I was surprised by the question, and the patient was surprised by my answer – we were in the middle of a telehealth visit. I realized that the common picture of telehealth conveys a complex process, perhaps similar to calling a customer service line.
Telehealth is typically arranged with your own doctor – same doctor, same relationship – just a different physical connection.
What about prescription refills?
Even if a clinic no longer has routine patient appointments, the office is probably still staffed. Patients can call the clinic and may also be able to request medication refills online.
Patients should check if their insurance company will allow 90-day supplies rather the usual 30 days so they can limit trips to the pharmacy. Some pharmacies are also providing medication delivery or curbside pickup now so high-risk patients don’t have to walk inside the store.
Staying on a diet
Diet is often one of the toughest adjustments needed for controlling chronic medical conditions.
Watching what we eat can be even more challenging during a pandemic. Following a low-carb diet for diabetes, following a low-salt diet for congestive heart failure or following a low-cholesterol diet for heart disease isn’t simple when people are sitting at home with stocked pantries and unable to get to the grocery store for fresh produce.
To avoid snacking out of boredom, try creating a daily meal and snack schedule.
If getting to the grocery store is a challenge, check if the store has senior-only hours, delivery or curbside pickup. A friend, neighbor or family member might be able to go grocery shopping for you. Many people are eager to help and just need to be asked.
Staying out of the hospital
Even if you don’t get COVID-19, it is still critically important that you continue to manage your chronic medical conditions.
When chronic conditions aren’t managed, patients run a higher risk of ending up in the emergency room and hospital – places where COVID-19 patients are likely also being treated and that have become overburdened amid the pandemic.
One of the best ways to help them is to take care of yourself. Stay home. Stay well. Stay connected.
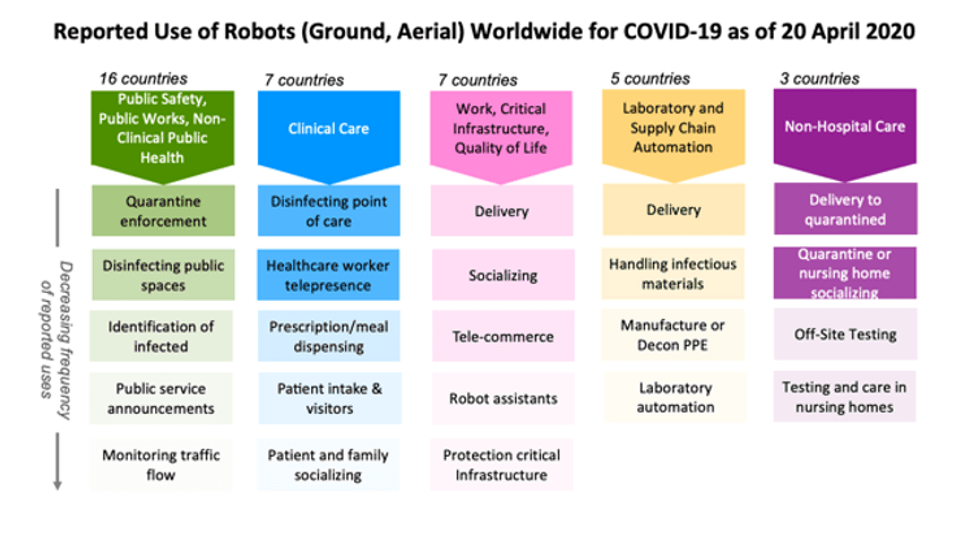
These are just a few of the two dozen ways robots have been used during the COVID-19 pandemic, from health care in and out of hospitals, automation of testing, supporting public safety and public works, to continuing daily work and life.
The lessons they’re teaching for the future are the same lessons learned at previous disasters but quickly forgotten as interest and funding faded. The best robots for a disaster are the robots, like those in these examples, that already exist in the health care and public safety sectors.
Research laboratories and startups are creating new robots, including one designed to allow health care workers to remotely take blood samples and perform mouth swabs. These prototypes are unlikely to make a difference now. However, the robots under development could make a difference in future disasters if momentum for robotics research continues.
Robots around the world
As roboticists at Texas A&M University and the Center for Robot-Assisted Search and Rescue, we examined over 120 press and social media reports from China, the U.S. and 19 other countries about how robots are being used during the COVID-19 pandemic. We found that ground and aerial robots are playing a notable role in almost every aspect of managing the crisis.
R. Murphy, V. Gandudi, Texas A&M J. Adams, Center for Robot-Assisted Search and Rescue, CC BY-ND
At work and home, robots are assisting in surprising ways. Realtors are teleoperating robots to show properties from the safety of their own homes. Workers building a new hospital in China were able work through the night because drones carried lighting. In Japan, students used robots to walk the stage for graduation, and in Cyprus, a person used a drone to walk his dog without violating stay-at-home restrictions.
Helping workers, not replacing them
Every disaster is different, but the experience of using robots for the COVID-19 pandemic presents an opportunity to finally learn three lessons documented over the past 20 years. One important lesson is that during a disaster robots do not replace people. They either perform tasks that a person could not do or do safely, or take on tasks that free up responders to handle the increased workload.
The majority of robots being used in hospitals treating COVID-19 patients have not replaced health care professionals. These robots are teleoperated, enabling the health care workers to apply their expertise and compassion to sick and isolated patients remotely.
A robot uses pulses of ultraviolet light to disinfect a hospital room in Johannesburg, South Africa.
A small number of robots are autonomous, such as the popular UVD decontamination robots and meal and prescription carts. But the reports indicate that the robots are not displacing workers. Instead, the robots are helping the existing hospital staff cope with the surge in infectious patients. The decontamination robots disinfect better and faster than human cleaners, while the carts reduce the amount of time and personal protective equipment nurses and aides must spend on ancillary tasks.
Off-the-shelf over prototypes
The second lesson is the robots used during an emergency are usually already in common use before the disaster. Technologists often rush out well-intentioned prototypes, but during an emergency, responders – health care workers and search-and-rescue teams – are too busy and stressed to learn to use something new and unfamiliar. They typically can’t absorb the unanticipated tasks and procedures, like having to frequently reboot or change batteries, that usually accompany new technology.
Fortunately, responders adopt technologies that their peers have used extensively and shown to work. For example, decontamination robots were already in daily use at many locations for preventing hospital-acquired infections. Sometimes responders also adapt existing robots. For example, agricultural drones designed for spraying pesticides in open fields are being adapted for spraying disinfectants in crowded urban cityscapes in China and India.
Workers in Kunming City, Yunnan Province, China refill a drone with disinfectant. The city is using drones to spray disinfectant in some public areas.
A third lesson follows from the second. Repurposing existing robots is generally more effective than building specialized prototypes. Building a new, specialized robot for a task takes years. Imagine trying to build a new kind of automobile from scratch. Even if such a car could be quickly designed and manufactured, only a few cars would be produced at first and they would likely lack the reliability, ease of use and safety that comes from months or years of feedback from continuous use.
Alternatively, a faster and more scalable approach is to modify existing cars or trucks. This is how robots are being configured for COVID-19 applications. For example, responders began using the thermal cameras already on bomb squad robots and drones – common in most large cities – to detect infected citizens running a high fever. While the jury is still out on whether thermal imaging is effective, the point is that existing public safety robots were rapidly repurposed for public health.
Don’t stockpile robots
The broad use of robots for COVID-19 is a strong indication that the health care system needed more robots, just like it needed more of everyday items such as personal protective equipment and ventilators. But while storing caches of hospital supplies makes sense, storing a cache of specialized robots for use in a future emergency does not.
This was the strategy of the nuclear power industry, and it failed during the Fukushima Daiichi nuclear accident. The robots stored by the Japanese Atomic Energy Agency for an emergency were outdated, and the operators were rusty or no longer employed. Instead, the Tokyo Electric Power Company lost valuable time acquiring and deploying commercial off-the-shelf bomb squad robots, which were in routine use throughout the world. While the commercial robots were not perfect for dealing with a radiological emergency, they were good enough and cheap enough for dozens of robots to be used throughout the facility.
Robots in future pandemics
Hopefully, COVID-19 will accelerate the adoption of existing robots and their adaptation to new niches, but it might also lead to new robots. Laboratory and supply chain automation is emerging as an overlooked opportunity. Automating the slow COVID-19 test processing that relies on a small set of labs and specially trained workers would eliminate some of the delays currently being experienced in many parts of the U.S.
Automation is not particularly exciting, but just like the unglamorous disinfecting robots in use now, it is a valuable application. If government and industry have finally learned the lessons from previous disasters, more mundane robots will be ready to work side by side with the health care workers on the front lines when the next pandemic arrives.
Every day the COVID-19 crisis reveals just how unprepared the U.S. health care system was.
But it’s not only the shortage of masks, tests and ventilators, nor our chaotic and contradictory public health response, evident across every level of government. COVID-19 has also brought into sharp relief how fragmented and disorganized the American health care system really is.
The U.S. system is often referred to as the dispersed model of care – less structured, with minimal central planning. This model encourages competition over collaboration. Indeed, many patients today can go directly to a specialist without consulting their primary care provider.
COVID-19 has shed light on these organizational problems – and the inability of our health care system to respond to growing demand. As an associate professor of health policy and management working on comparative health systems reforms, I’d like to highlight what primary care can offer in the U.S., especially in the context of a crisis like this one.
Primary care physicians can provide tremendous front-line support during the pandemic.
While being able to go directly to a specialist may sound like a good deal for the patient, this model has downsides, including higher costs.
That’s in part due to the fact that specialists stay in business by performing diagnostic examinations such as MRI examinations, and surgical procedures, such as coronary artery bypass grafts. And, these specialists compete with each other and try to maximize revenue. The health care industry as a whole spent US$30 billion on advertising. This competitive model encourages provision of high cost services at a higher volume.
These services are not only expensive but are also associated with higher rates of complications and avoidable hospital admissions and readmissions as well as higher rates of hospital-acquired infections. All of these factors point to waste and major inefficiencies in the health care provision and a lack of communication between providers.
How primary care doctors would help
In the current crisis, governors, health officials and the public have placed much attention on 911 and hospital bed capacity. Cities and state governments are coming up with their own response plans without much support from public health agencies and federal government. One example: A fire department battalion chief in Paterson, New Jersey, responded to 911 calls in person to assess possible COVID-19 cases; he determined whether a specialized ambulance should follow up.
Primary care providers could support this triaging work on the front lines and possibly save lives. They also could identify and contact high-risk patients and educate them about the symptoms of COVID-19 before they get sick. They could facilitate at-home testing – of course, depending on the availability of tests. If patients have COVID-19, primary care doctors can manage their care at home through telemedicine or by phone, and refer to hospitals when they get worse.
As the crisis deepens and then abates, primary care doctors will need to educate their patients and encourage behaviors that prevent the spread of disease. And, they can also play a key role for recovering patients in care teams deciding the discharge procedures and help integrate with social care services. These would be essential services for recovering nursing home residents or homeless individuals.
When the system blocks care
But because of our dispersed model, many people don’t even have a primary care doctor. And for those of us who do have them, there is no guarantee that we will be able to receive much needed services.
Some practices are struggling to remain open, due to staff shortages and financial difficulties, while others change their delivery practices such as switching to telemedicine or canceling well and chronic care visits to accommodate need.
A recent survey by Primary Care Collaborative, conducted April 3-6, 2020 with more than 1,000 primary care physicians, nurse practitioners and physician assistants, shows primary care services are “dangerously under-resourced”: 58% of participants report the use of used and homemade personal protective equipment at their practice, while 29% of clinicians report no capacity for COVID-19 testing and 39% have only limited capacity. Nearly half of practices have clinical care team members out sick or quarantined, while 40% report their clinical staff being redeployed within the health system.
The use of telemedicine is growing, but 72% of clinicians reported that “patients most vulnerable do not have capabilities for virtual visits” due to not having a computer or internet access. In addition, 43% of participating clinicians revealed tremendous financial strains threatening practice closure. Especially small, independent practices are struggling with a severe drop in visits, and close to 60% are not sure the majority of care they are provided is reimbursable.
Similarly, community health centers that provide care to medically underserved urban and rural communities are struggling to survive.
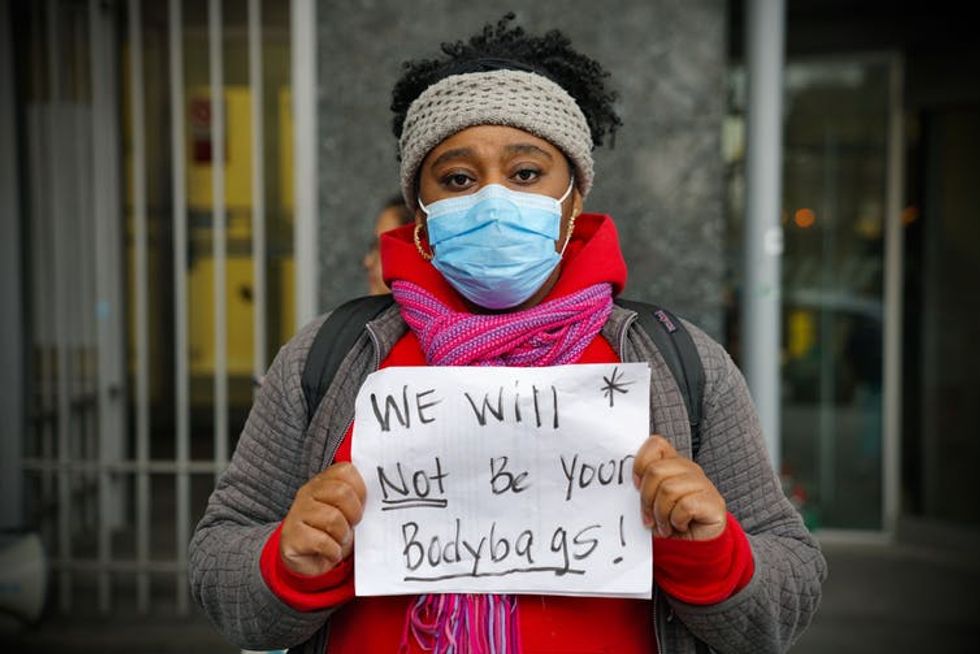
In Harlem, New York, nurses and health care workers protest for more personal protective equipment and safer working conditions. The shortages, says the author, are indicative of an inefficient health care system.
I do not think that these are just small hiccups. Rather, I think these are the reasons we urgently need a renewed debate on universal health coverage, with primary care as its cornerstone.
Various analogies have been used to describe primary care providers, ranging from gatekeepers to quarterbacks. I would suggest another familiar analogy - that of a large, shiny building representing the American health care system. Primary care is often considered as one of the pillars holding the building or the foundation that addresses majority of the health care needs and refers patients to higher levels for complex cases. I would like to add that primary care is also the control center in charge of ensuring an integrated, people-centered system of care.
Primary care system in the U.S. needs to be supported with an organized response that protects the workforce, ensures financial sustainability and facilitates access to accurate information.
To focus on their care management and integration responsibilities, primary care providers need assistance to field questions about COVID-19 symptoms and triaging patients. There are some initiatives we can learn from such as the British health care system’s NHS911 hotline or COVID-19 Connected Care Center created in partnership with the Oregon Health & Science University in the U.S.
Our COVID-19 response does not have to be another instance of the “rediscovery of the deficiencies and promises” of our medical and public health systems, but instead, a system-building effort that will better serve us during times of crisis.