County executives in Utah this week called out two local businesses for putting their employees' health at risk by telling them to ignore quarantine guidelines.
The Utah Daily Herald reports that Utah County Commissioners Tanner Ainge, Bill Lee and Nathan Ivie wrote a letter this week in which they revealed 48 percent of workers at an unidentified local business had come down sick with COVID-19 after they encouraged them to blow off social distancing and other restrictions.
In fact, the commissioners say that this business actually ordered people who got sick to keep coming to their jobs.
"During the tracing contacts conducted by the Utah County Health Department and Utah Department of Utah, we found these businesses instructed employees to not follow quarantine guidelines after exposure to a confirmed case at work and required employees with a confirmed COVID-19 diagnosis to still report to work,” the statement said. “This is completely unacceptable and resulted in a temporary full closure for one business along with heightened requirements for future cleaning and inspections."
The officials have nonetheless declined so far to name the businesses that have defied guidelines.
Secretary of State Mike Pompeo has been making bold assertions about COVID-19 being released from a lab in China, despite the fact that other allied intelligence agencies have said otherwise.
During a press conference on Wednesday, a reporter asked Pompeo what he made of intelligence officials in United Kingdom, Canada, Australia and New Zealand stating that it is "unlikely" that COVID-19 came from a lab, and the secretary of state angrily attacked her.
"Your efforts to spend your whole life trying to drive a little wedge between senior American officials, it's just, it's just, it's just false!" Pompeo fumed.
"We think it's highly unlikely it was an accident," a Western diplomatic official with knowledge of the intelligence said. "It is highly likely it was naturally occurring and that the human infection was from natural human and animal interaction."
Pro-Trump Evangelist Franklin Graham is blasting stay-at-home policies around the country and warning Americans “our future and our freedoms” could be in danger.
In a series of rants attacking Democrats and the media, the Christian evangelist, missionary, and highly-paid non-profit CEO told his 8.5 million Facebook followers that even though the coronavirus is dangerous, they should not be afraid because everyone is going to die.
“Each one of us will have to meet death,” Graham wrote on Saturday. “With the dark storm clouds of COVID-19 still hanging low, we need to go on with living our lives and doing our work, while taking personal responsibility. Social distancing, hand washing, wearing masks in public places—all of these precautions are important.”
That same day Graham showed his commitment to social distancing and mask-wearing:
He went on to spread an anti-Trump conspiracy theory, saying, “fear and anxiety can be very detrimental to one’s health as well. No matter how negative the reports are from the media and liberal politicians who want to use the coronavirus to destroy President Donald J. Trump, if we put our faith and trust in Jesus Christ, we don’t have to be afraid. God made us. He has a plan and a purpose for our lives, and He knows the number of our days.”
“I am of the opinion that keeping the economy shut down, is doing more damage to people’s lives than COVID-19. In the 60,000+ deaths from COVID-19 nationwide, the majority had underlying health issues, which is true in Italy as well. It is estimated that heart disease will take the lives of 640,000 people across our country this year and cancer is expected to claim over 600,000 lives as well. One thing is 100% certain—we will all die.”
“Many in the left-leaning media want to project the worse-case scenarios relating to COVID-19. It makes great headlines for them—and it produces fear in the public. A recent CNN headline said that the new coronavirus is likely to keep spreading for another 18-24 months, giving ammunition to liberal states who want to keep businesses closed. I agree that COVID-19 may be around for a while—human coronavirus has already been around in some form for many years. But as a nation and as individuals, we have to learn to live with pandemics, whether it’s coronavirus or any other. We can’t hide in a cave until the world is free from every virus or threat.”
“Here we go again. Another headline by CNN to try to put fear in the minds of readers. What happens if a coronavirus vaccine is never developed? The ‘what-ifs’ could be endless. What if the sky fell tomorrow? There are a lot of hypotheticals being thrown out there that are intended to scare people,” Graham claimed, confusing scientific analysis with fear-mongering.
And in words giving ammunition to stay-at-home protestors and others who dispute the government’s power in health emergencies, Graham falsely suggested stay-at-home policies might be unconstitutional.
“It’s becoming more obvious to people that the response of some in the government is not just about protecting lives, but it’s about control. Never before in our history have those who are well been quarantined rather than those who are sick! I don’t want to minimize the fact that the coronavirus is dangerous. We need to take precautions and we need to exercise personal responsibility. But we also need to be cautious before we say yes to every ban proposed and agree to anything that we think might help protect us from the virus, to make sure that we’re not letting go of some of our constitutional rights. Our response to the coronavirus pandemic could greatly affect our future and our freedoms.”
Charlie Sykes, who for decades was a right-wing talk radio show host in Wisconsin, is taking many of his former allies to task for their crusade against public health measures intended to stop the spread of COVID-19.
In a column at The Bulwark entitled "A Pandemic of Madness," Sykes calls out protesters and Fox News hosts who are urging people to rebel against wearing face masks and social distancing during a pandemic that so far has killed more than 71,000 Americans in less than two months.
"The mood has been set from the top, as Trump has pivoted," Sykes writes. "The result is a pandemic of confusion and madness, where mixed signals, conspiracy theories, paranoia, and tribal loyalties clash with common sense medical practices."
He then details how anti-face mask activism has taken off like wildfire throughout the country.
"In Stillwater, Oklahoma, city officials had to quickly back off an order requiring the wearing of face masks, after threats of violence against employees of private firms who tried to enforce it," Sykes writes. "Ohio also had to back off a similar mask order after pushback as well."
He also singles out Fox News host Laura Ingraham for turning public safety into a culture war.
"Fox News hosts kept up the drumbeat," he writes. "While Sean Hannity came out against armed protests, Laura Ingraham continues to disseminate bogus death counts, peddle her favorite malaria-drug, and criticize 'social distancing.'"
MIAMI — It was March 1 when Florida announced its first two cases of the novel coronavirus, a 29-year-old Hillsborough County woman who had traveled to Italy and a 63-year-old Manatee County man. But buried in data recently published by the Florida health department is an intriguing revelation: The spread of COVID-19 in Florida likely began in January, if not earlier. State health officials have documented at least 170 COVID-19 patients reporting symptoms between Dec. 31, 2019, and February 29, according to a Miami Herald analysis of state health data. Of them, 40% had no apparent contact with ...
"He absolutely does not want you to view these deaths for what they are... a result of his abject failure to handle the pandemic in any logical way."
President Donald Trump made clear during both an interview and a press briefing Tuesday that he is willing to sacrifice lives for the sake of reopening U.S. businesses amid the coronavirus pandemic, declaring that jumpstarting the American economy is worth the dire public health risks.
"There'll be more death," Trump said in an appearance on ABCNews. "I think we're doing very well on the vaccines but, with or without a vaccine, it's going to pass, and we're going to be back to normal."
The president said it is possible that there will be an increase in the U.S. death toll "because you won't be locked into an apartment or house or whatever it is."
"We have to get our country back," Trump added. "You know, people are dying the other way too."
WATCH:
Trump's comments came a day after an internal Centers for Disease Control and Prevention document projected that the daily Covid-19 death toll in the U.S. could rise to 3,000 by June, nearly double the current rate. Despite warnings from public health officials and the lack of adequate testing, a number of states are taking steps to reopen their economies with the backing of the president.
Two anonymous Trump administration officials toldCNN that new fatality projections "are not currently expected to affect the White House's plans for reopening the country."
In a press briefing on Tuesday, Trump said he views "our great citizens of this country to a certain extent and to a large extent as warriors."
"They're warriors," the president continued. "We can't keep our country closed. We have to open our country... Will some people be affected? Yes. Will some people be affected badly? Yes. But we have to get our country open."
"I think the term here is 'cannon fodder,'" Vox's David Roberts tweeted in response to Trump's "warrior" comments.
Kim Nelson, a public health advocate and South Carolina Democratic congressional candidate, argued that Trump is characterizing people whose lives are at risk as warriors "so that you'll view those who died as having sacrificed for the greater good."
"He absolutely does not want you to view these deaths for what they are... a result of his abject failure to handle the pandemic in any logical way," Nelson tweeted.
Editor’s Note: As researchers try to find treatments and create a vaccine for COVID-19, doctors and others on the front lines continue to find perplexing symptoms. And the disease itself has unpredictable effects on various people. Dr. William Petri, a professor of medicine at the University of Virginia Medical School, answers questions about these confusing findings.
Some evidence suggests that patients experience low oxygen saturation days before they appear in the ER. If so, is there a way to treat patients earlier?
Even before symptoms arise, people infected with SARS-CoV-2 show damage to their lungs. This is likely why low oxygen saturation – that is, below-normal oxygen levels in their blood – occurs before the patient goes to the ER. Restoring those levels to normal is presumed, though not proven, to be beneficial; giving patients supplemental oxygen via a nasal cannula, a flexible tube that delivers oxygen, placed just inside the nostrils, will restore oxygen to normal levels unless disease worsens to the extent that mechanical ventilation is needed.
Young adults are having strokes with COVID-19. Does this suggest the illness is more of a vascular disease than a lung disease in that age group?
COVID-19 can be a devastating disease to multiple organs and systems in the body, including the vascular and immune systems. A lung infection is the primary cause of disease and death. There are examples of the clotting system being activated and causing strokes, perhaps caused by an immune system responding abnormally to COVID-19.
A sign in a clothing store in Stuart, Florida warns shoppers to keep their distance. Retail stores, restaurants and beaches have now reopened in a majority of Florida counties.
The Centers for Disease Control and Prevention recently updated its official list of symptoms. Does this suggest anything unusual about COVID-19?
This new information is due to a greater number of infected individuals being studied. The update simply reflects a better understanding of the full spectrum of illness due to COVID-19, from asymptomatic to presymptomatic to severe and fatal
infections.
How can so many people experience such mild symptoms and others quickly die from it?
One of the most fascinating aspects of these diseases is the huge difference that individuals experience with an infection. In our own research, we have found that many children in the U.S. infected with cryptosporidia have no symptoms, yet this parasite is a major killer of infants in the developing world. After an infection of SARS-CoV-2, the severity of the illness is likely due in part to how the patient’s immune system responds; an overzealous immune response may cause death through what is called colloquially a “cytokine storm..” We do not know yet if cytokine storms occur more in one group than another – for example, older versus younger.
Thousands of white markers on the grounds of the First Congregational Church in Greenwich, Connecticut. Each marker honors lives lost to the COVID-19 pandemic.
The disease appears now to affect various other organs – heart and kidney, for example. What does this suggest?
What we know most clearly is that infection starts only in human cells with the ACE2 receptor – that is, in a cell that is capable of receiving the virus. That is present not only in the lungs, but in other cells as well, including those in the intestine and in the nasal mucosa, which lines the nasal cavity. When those cells are infected, the immune system is activated. A consequence is that both the heart and kidney are affected.
Why are some countries not experiencing as much COVID-19 as the U.S., Europe and China?
I think it’s too early in the pandemic to know if certain countries or populations are relatively less susceptible. The younger overall age of a population could be a primary factor. Or perhaps the virus, so far at least, has not had time to spread more widely in these countries.
With the FDA approving Gilead’s Remdesivir as an emergency use treatment for the most acute cases of COVID-19, many people are wondering what type of a drug it is.
Remdesivir is a member of one of the oldest and most important classes of drugs – known as nucleoside analogue. Currently there are more than 30 of these types of drugs that have been approved for use in treating viruses, cancers, parasites, as well as bacterial and fungal infections, with many more currently in clinical and preclinical trials.
I am a medicinal chemist who has worked in design and synthesis of these important drug treatments for over 30 years. I have written numerous reviews over the years about these drugs and their structure and function, and as a result have had many inquiries lately from friends, family and others not in the field asking me to explain what exactly is it about Remdesivir that makes it so effective, but also why it is so interesting. Understanding why means digging into the biochemistry of this class of drugs.
Fake genetic building blocks
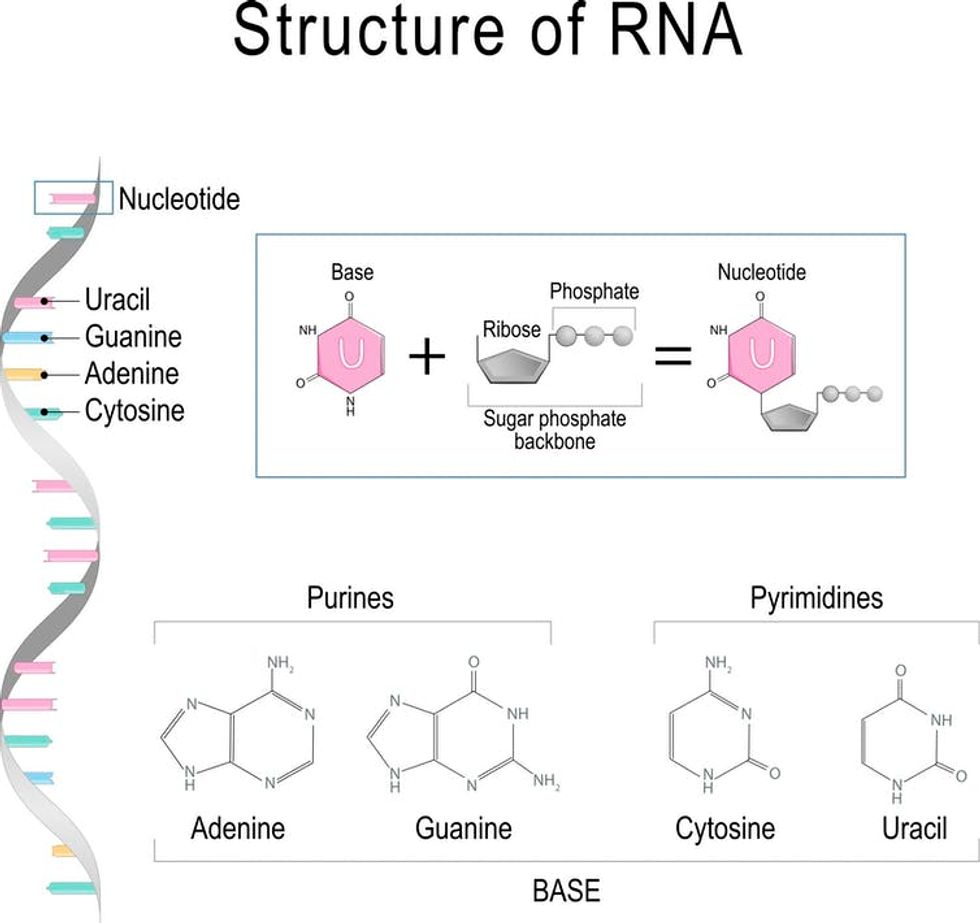
The reason nucleoside analogues and a similar group called nucleotide analogues are so effective is that they resemble the naturally occurring molecules known as nucleosides – cytidine, thymidine, uridine, guanosine and adenosine. These are the essential building blocks for the DNA and RNA that carry our genetic information and play critical roles in our body’s biological processes.
Slight differences in the chemical structure of these analogues from naturally occurring compounds make them effective as drugs. If an organism like a virus incorporates a nucleoside analogue into its genetic material, rather than the real thing, even small changes to the structure of these building blocks prevent the regular chemistry from happening and ultimately foils the ability of the virus to replicate.
The basic structure of a nucleoside includes a sugar group and a base (A, C, G, T or U), and in the case of a nucleotide, a group containing a phosphate which is a collection of oxygen and phosphorus atoms.
Every building block of DNA is made from three parts: a sugar, a base (A, C, G, or T) and a phosphate group. Every building block of RNA is made from (A, C, G, or U).
ttsz / Getty Images
The first nucleoside analogues were approved for medicinal use in the 1950s. The early nucleosides had only simple modifications, typically either to the sugar or the base, while today’s nucleosides, such as Remdesivir, typically have several modifications to their structure. These modifications are essential to their therapeutic activity.
How does Remdesivir work as antiviral therapeutic?
This activity occurs because nucleoside/tide analogues mimic the structure of a natural nucleoside or nucleotide such that they are recognized by, for example, viruses. Due to those structural modifications, however, they stop or interrupt viral replication, which stops the virus from multiplying and infecting more cells in the body.
As a result, they are known as direct-acting antivirals, and this is the case for Remdesivir, which works by blocking the coronavirus’s RNA polymerase – one of the key enzymes that this virus needs to replicate its genetic material (RNA) and proliferate in our bodies. Remdesivir works when the enzyme replicating the genetic material for a new generation of viruses accidentally grabs this nucleoside analogue rather than the natural molecule and incorporates it into the growing RNA strand. Doing this essentially blocks the rest of the RNA from being replicated; this in turn prevents the virus from multiplying.
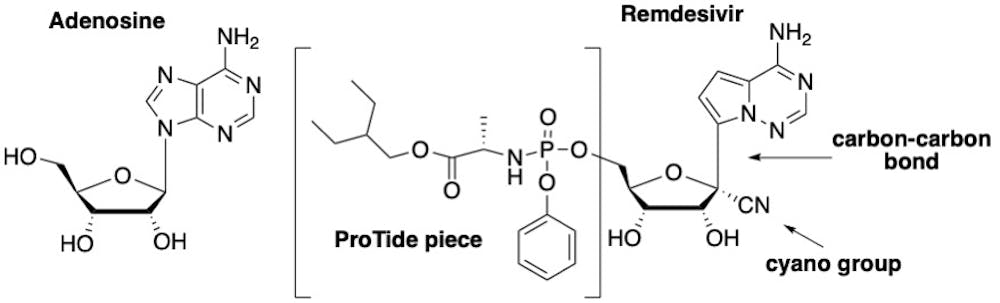
The drug Remdesivir is basically an altered version of the natural building block adenosine – which is essential for DNA and RNA. Comparing the structure of Remdesivir with adenosine, one can see there are three key modifications that make it effective.
The first is that Remdesivir, as it is administered, is not the actual active drug; it is actually a “prodrug,” meaning it must be modified once in the body before it becomes an active drug. Prodrugs are used for many reasons, including protecting a drug until it reaches its site of action. The active form of Remdesivir contains three phosphate groups; it is this form that is recognized by the virus’s RNA polymerase enzyme.
A naturally occurring nucleotide (left) which is a building block of RNA and DNA and Remdesivir (right) which is a variation on its natural counterpart.
The second important modification on Remdesivir is the carbon-nitrogen (CN) group attached to the sugar. Once Remdesivir is incorporated into the RNA growing chain, the presence of this CN group causes the shape of the sugar to pucker, which, in turn, distorts the shape of the RNA strand such that only three more nucleotides can be added. This terminates the production of the RNA strand and is what ultimately sabotages the replication of the virus.
The third important structural feature which makes Remdesivir differ from adenosine is the change of one particular chemical bond on the molecule. Rather than a bond linking a carbon and nitrogen atoms, chemists replaced the nitrogen with another carbon, creating a carbon-carbon bond. This is critical to the success of this drug because coronaviruses have a special enzyme that recognizes unnatural nucleosides and clips them out. But by changing this chemical bond, Remdesivir cannot be removed by the enzyme, allowing it to stay in the growing chain and block replication.
Remdesivir trials
Remdesivir originally was found during a drug discovery program at Gilead to search for inhibitors of the hepatitis C virus, which is another RNA virus. Although Gilead ultimately selected a different nucleoside analogue for treatment of hepatitis the company tested the drug to see if it was effective against other RNA viruses. Remdesivir exhibited potent activity against Ebola and Middle Eastern respiratory virus, among others.
According to the NIH, patients who received Remdesivir had a faster recovery compared to those who received placebo; 11 days compared with 15 days for those who received the placebo. “Results also suggested a survival benefit, with a mortality rate of 8.0% for the group receiving Remdesivir versus 11.6% for the placebo group,” according to the NIH press release.
While these results are preliminary, there are a plethora of clinical trials underway across the world. Regardless, a certain amount of caution is still needed. As noted by Dr. Anthony Fauci on NBC’s “Today” show, “the antiviral drug Remdesivir is the first step in what we project will be better and better drugs coming along” to treat COVID-19, but cautioned, “This is not the total answer.”
I share this view with many other scientists in the field. No matter what those results ultimately show, Remdesivir will mostly certainly be part of a cocktail of drugs, just as is standard for treating other viruses such as HIV and hepatitis C.
A combination, or cocktail, of drugs will provide a more effective and more complete therapy that blocks the virus from replicating. The other benefit of such a drug cocktail is that it lowers the chance the virus will develop resistance to the therapy. In the meantime, these early results for Remdesivir are proving to be an important source of hope for many of us across the world as we wait for this pandemic to subside.
As Iowa Gov. Kim Reynolds put it in a press conference, virus outbreaks in packing plants are “very difficult to contain.” But what makes these plants so dangerous? As a sociologist who has studied food system labor issues, I see two answers.
First, working conditions experienced in meatpacking plants, which are shaped by the pressures of efficient production, contribute to the spread of COVID-19. Second, this industry has evolved since the mid-20th century in ways that make it hard for workers to advocate for safe conditions even in good times, let alone during a pandemic.
Together, these factors help to explain why U.S. meatpacking plants are so dangerous now – and why this problem will be difficult to solve.
Employees at large meatpacking plants say they don’t feel safe from COVID-19.
A hard job in good times
The meatpacking industry is an important job source for thousands of people. In 2019 it employed nearly 200,000 people in direct meat processing jobs at wages averaging US$14.13 per hour or $29,400 yearly.
Even in normal conditions, meatpacking plants are risky places to work. The job requires using knives, saws and other cutting tools, as well as operating industrial meat grinders and other heavy machinery.
Traumatic injuries due to workplace accidents are common, and mistakes can have gruesome consequences. Government researchers have also documented chronic injuries, such as repetitive motion strains, among packing plant workers.
The same conditions that lead to these accidents and injuries during normal times also contribute to the spread of coronavirus. To understand this connection, it is first important to know that meatpacking is a volume industry. The higher a plant’s daily throughput – that is, the more animals it turns into meat – the more lucrative it is.
For instance, one Smithfield plant in Sioux Falls, South Dakota, which shut down indefinitely in April after hundreds of workers tested positive for COVID-19, employed 3,700 people and produced 18 million servings of pork daily.
To maximize efficiency, production takes place on an assembly line – or more accurately, a disassembly line. Workers stand close together and perform simple, repetitive tasks on animal parts as the parts stream by.
The speed and organization of meatpacking both promote the spread of coronavirus. Employees labor alongside one another, working at a rate that makes it difficult, if not impossible, to practice protective behaviors such as covering sneezes and coughs.
The Centers for Disease Control and Prevention has issued guidelines to allow meatpacking workers to continue working during the pandemic. They include spacing workers at least six feet apart and installing barriers between them. Some plants have adopted these controls, but the pressures of rapid production may well limit their effectiveness.
Meat processing stations at the JBS Beef Plant in Greeley, Colo., equipped with new sheet-metal partitions, April 23, 2020. As of early May 2020 the plant had recorded more than 200 confirmed cases of COVID-19 and 6 employee deaths.
Understanding why meatpacking workers tolerate these difficult and dangerous conditions requires a look at the industry’s history.
Many people assume that jobs in packing plants have always been as difficult and dangerous as those depicted in journalist Upton Sinclair’s famed 1906 novel “The Jungle.” That book described meatpacking workers in early 20th-century Chicago facing similar conditions to those in the modern industry.
But this assumption conceals an important story. For several decades after World War II, conditions in meatpacking plants steadily improved as a result of pressure from workers themselves.
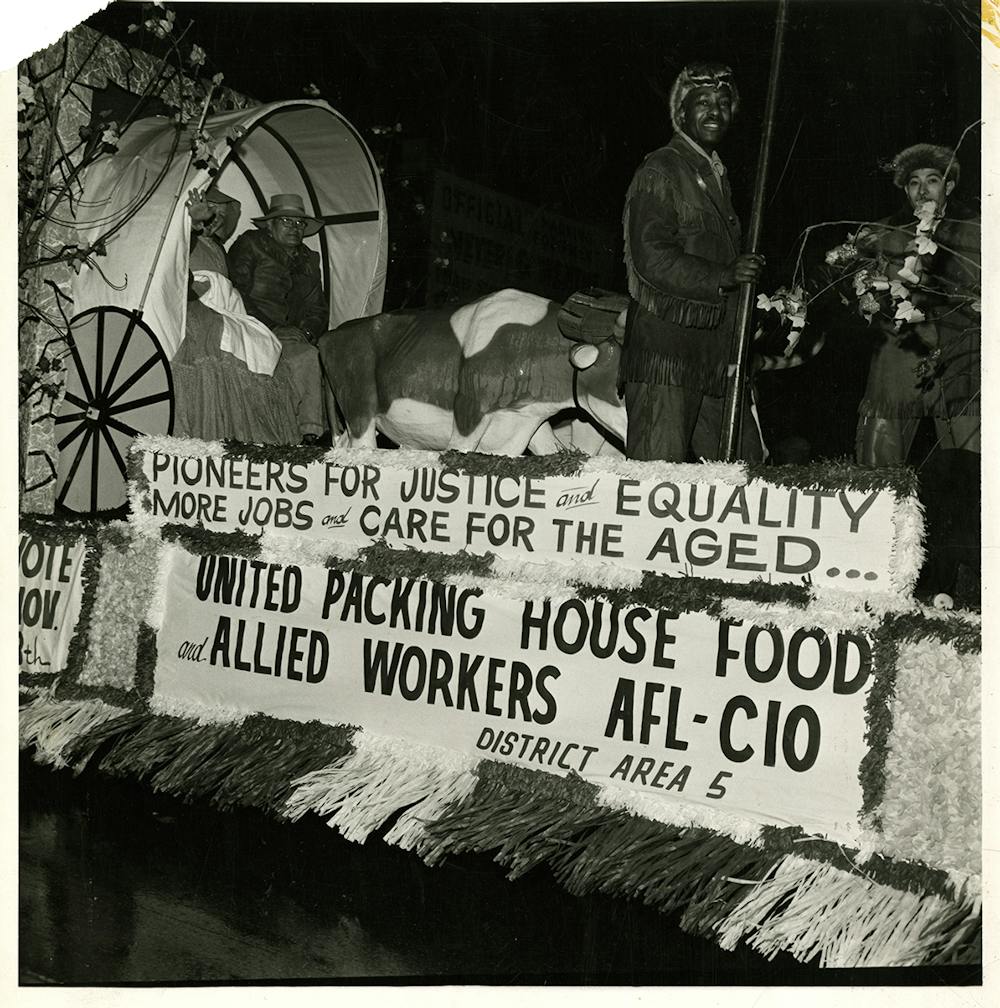
Starting in 1943, the United Packinghouse Workers of America, a labor union, organized meatpacking employees in major cities. At the height of its influence, this union secured “master agreements” with the largest firms, such as Armour and Swift, ensuring standard wages and working conditions across the industry.
One source of the UPWA’s influence was its ability to build interracial alliances. Racial antagonism between black and white workers, linked to job discrimination and the use of black workers to break strikes in the early 20th century, had historically undermined union efforts in meatpacking plants.
UPWA District Area 5 Members Parade float, circa 1960, Chicago.
The union’s logo, which depicted clasped black and white hands, symbolized its ability to bridge these differences. Its support for the civil rights movement in the 1960s also revealed its commitment to racial equality.
A changing labor force
But by the 1970s, the union was in decline. A key factor was industry leaders’ decision to shift production from cities with a strong union tradition, like Chicago and Kansas City, to small towns scattered across the Great Plains and the southeastern United States.
Rural work forces are more difficult to organize than their urban counterparts for many reasons. Most small towns do not have a history of union activity, and anti-union sentiment is often strong – as shown by the prevalence of right-to-work laws in many rural states.
Moreover, packing plants are often small towns’ only major employers. Workers and municipal authorities alike depend on plants for jobs and tax revenue. This relationship creates enormous pressure to treat meat processing companies with deference.
Additionally, meatpacking consolidated in the late 20th century. Plants grew larger, and a relative handful of firms such as Cargill and Tyson came to dominate processing of beef, poultry and other meats. Consolidation gives these firms greater ability to control working conditions and wages.
Finally, today’s plants often recruit workers from Mexico and Central America, some of whom may lack legal authorization to work in the U.S. They also hire refugees who may be unfamiliar with U.S. labor protections and have few other employment possibilities.
These workers’ precarious legal and economic standing makes it hard for them to challenge employers. Cultural differences, language gaps and racial prejudice can also pose obstacles to collective action.
The challenge of coronavirus
Workers’ organizations have not disappeared. The United Food and Commercial Workers Union has called on the Trump administration to ensure safety during the pandemic, but it is fighting an uphill battle.
Despite President Trump’s reassurances that closed plants will reopen safely, I expect that the pressures of efficiency and limits on workers’ ability to advocate for themselves will cause infections to persist.
In meatpacking as in other industries, the pandemic has revealed how people who do “essential” work for Americans can be treated as if they are expendable.
It has been less than two months since the world scrambled to go into the “Great Lockdown” to slow the spread of COVID-19. Now, many countries are considering their exit strategies. Some have already eased up.
The push is largely economic. There is a lot scientists don’t yet understand about the novel coronavirus, and there is no known cure or vaccine. Many countries are still experiencing a rise in infections. But the lockdowns have played havoc with people’s livelihoods. Entire economies are in meltdown: The International Monetary Fund predicts the worst economic downturn since the Great Depression.
Just as each nation chose a different route into lockdown, each is likely to choose its own exit path. I have launched a research initiative, “Imagining a Digital Economy for All 2030,” with a focus on the post-pandemic global economy. We have been studying the characteristics of 40 countries that help explain how governments and citizens have acted to contain the COVID-19 outbreak and their preparedness to take an economy online. Our analysis offers ways to gauge which countries are best prepared for a safe exit.
It seems clear that the safest idea is to reopen slowly, in phases, while remaining ready to reenter lockdown in case of new outbreaks. By looking at how well a nation managed the first wave of the pandemic, and how ready it is to work remotely by falling back onto the online economy, we now understand how prepared nations are to restart economic activity without triggering fresh rounds of public health disasters.
Public health and technology
Not every country is well equipped to ease itself out of a lockdown safely.
A nation’s ability to manage the outbreak relies on many factors: the willingness of governments to take decisive action; citizen compliance in staying home and social distancing; and capacity for adequate testing for the disease, including “contact tracing” – tracking down the people who have been in contact with those infected. Those characteristics are also key to managing future outbreaks.
In parallel, not every country is ready to shift much of its economic activity online. Around the world, not everyone has affordable, reliable internet service; or the jobs, devices and digital apps that would let them work productively from home; or ways to make payments and get public services online. In some countries – though not all – workers who can’t do their jobs remotely can reduce their in-person contact by using digital transactions, whether it is for carry-out food, e-commerce or receiving bailout checks and unemployment benefits.
Countries such as Germany, New Zealand and South Korea are strong in both disease-fighting and digital-economy preparedness. Their economic activity isn’t as dependent on in-person interactions, and authorities can respond quickly if loosened rules result in a spike in cases. In contrast, the U.S., Italy and Japan face different challenges before they can safely lift lockdowns.
Japanese residents enjoy a beach while wearing masks and staying apart from each other, as Japan’s emergency lockdown continues.
The results are evident in the mortality rates in the U.S. and other, better-prepared countries: On May 5, the key statistic shows the U.S. death rate was more than three times that of Germany, nearly 200 times those in New Zealand and South Korea.
What made the difference?
The countries that more efficiently managed this first outbreak and its consequences capitalized on their public health preparation to get a grip on the infection quickly. Germany has a high volume of infections but low mortality. The country only knows this because it had tested extensively – at a rate of 21 people per 1,000, as compared with 9.8 per 1,000 in the U.S.
South Korea, while among the earliest countries affected, kept its mortality among the lowest in the world through widespread testing and deploying technology for widespread contact tracing. Infected individuals’ interactions were retraced using cellphone location data, surveillance camera footage and credit card records. Websites and apps offer details on infected people’s travel and exposure risks.
Italy initially underestimated the severity of its outbreak, but then imposed a strict lockdown with high citizen compliance and widespread testing and tracing. However, we found in our study that Italy is among the least prepared European Union members for a shift to a digital economy. Germany, New Zealand and South Korea all have higher levels of internet access and service, digital payments and public services, and employers ready to handle remote work.
Japan’s situation is particularly challenging because it eased up its restrictions too early and then had to impose an emergency to stem additional outbreaks. It is also relatively unprepared in digital terms because of a host of factors, ranging from peer pressure to come into the office, to security concerns, transactions that require a paper trail, often requiring official corporate seals, missing digital infrastructure and a continued aversion to digital payments.
Each of these countries is a wealthy, developed nation, so the differences are not due to affordability. Our research has found that preparedness requires not just funding but also farsighted, credible and transparent leadership and citizens’ trust in that leadership. The first leads to timely and firm decisions, and the second contributes to citizens’ willingness to cooperate with those decisions.
For instance, German Chancellor Angela Merkel’s background as a trained scientist gave her powerful credibility when facing a scientific crisis. New Zealand Prime Minister Jacinda Ardern clearly explained her “go early, go hard” approach to lockdown restrictions, and her citizens agreed. In South Korea, authorities controlled the virus through “decisive and transparent leadership based on data, not emotion.”
As governments seek their own exit pathways, and aim to strengthen areas where they are weak, there’s no way to be completely certain or fully prepared for what might happen next.
In our research, we’ve found one principle that governments might find useful to guide them through the uncertainty. It’s from a former New Zealand prime minister, Helen Clark: “Economies can recover; the dead can’t.”
The COVID-19 crisis has demonstrated the degree to which we depend on the work of others. This is particularly true of essential workers like truck drivers, grocery store employees and hospital nurses who are ensuring the rest of us stay safe and are able to get the supplies, food and health care we need.
The pandemic has also drawn attention to the fact that these workers, like all Americans, do not receive many of the basic workplace benefits and protections – like paid sick leave and basic health care – that workers in almost every other developed country in the world receive as a matter of course.
The Families First Coronavirus Response Act, passed by Congress in March, provides two weeks of leave for workers who fall ill from COVID-19 but is riddled with exceptions and covers very few essential workers. Some lawmakers hope to remedy this with the “Essential Workers Bill of Rights,” which would ensure that about 60 million workers receive 10 benefits during the crisis, including paid sick leave, hazard pay, no-cost health care coverage and collective bargaining protections.
While the measure’s odds of passage are low, even if it becomes law it would only temporarily address the problem for some workers. Once the pandemic ends, much of the American workforce will still be without basic benefits and protections taken for granted in virtually every other developed country.
I’m a labor scholar who has been studying employment relations for 40 years. I believe there are three “rights” in the bill that are especially urgent.
Paid sick leave
Over 33 million U.S. workers – almost a quarter of the workforce – do not have access to paid sick leave. The problem is especially bad for the lowest-paid employees, many of whom are essential workers.
As a result, up to 90% of employees have reported that they sometimes go to work when ill to prevent losing a day’s pay or being disciplined or fired.
This is problematic for both employees and employers, particularly when workers are suffering from colds, flu or other viral illnesses that are easily spread by person-to-person contact. It’s also been seen as a contributing factor to the current COVID-19 crisis.
A study of 22 developed countries found that the average number of paid sick days required was 28. Excluding the U.S.‘s zero days, policies ranged from a low of five in New Zealand to 50 in Norway.
Free health care
The pandemic has also drawn attention to just how many Americans, including essential workers, lack basic health care.
Over 10% of non-elderly Americans – about 28 million individuals – didn’t have health insurance in 2018. Another 29% of adults were underinsured, meaning they have high deductibles and out-of-pocket medical expenses relative to their income. Lower-paid workers generally pay higher deductibles than their higher-earning counterparts.
One of the key reasons so many American workers do not have paid sick leave or health care is that the U.S. differs from most developed nations in another crucial way: the low share of employees who belong to unions.
But in 2019, only 8.3% of nurse aides, housekeepers and other health care support workers in the U.S. were represented by a union. For registered nurses, therapists and physicians, that figure was 13.7%. By comparison, 38% of workers in the health care industry in the U.K. and 80% to 85% of health care workers in Sweden are represented by unions.
And U.S. protections for those who try to organize a union are generally the weakest among developed nations. A study that rated countries’ legal protections for workers on a 1-to-5 scale from best to worst gave the U.S. a 4 because employers were found to have “engaged in serious efforts to crush the collective voice of workers.” The U.S. shared that category with Iran, Iraq, Haiti and Honduras.
Giving essential workers these and other benefits would clearly help them worry less about what happens if they get sick and more about the important jobs they are doing for all of us during the pandemic. And doing the same for all U.S. workers on a permanent basis would make us more prepared for the next one.
On Tuesday, state Reps. Steve Toth and Briscoe Cain sat wearing barbers' gowns in a Houston-area salon, ready for their haircuts. Both Republicans were breaking state law by doing so, but to them, it mattered no less — one was there to send a message to Gov. Greg Abbott, and the other was there as an act of civil disobedience.
“A little less on the sides,” Toth, from The Woodlands, told the hairstylist while on the phone with a Texas Tribune reporter, noting that "there's absolutely no reason" why such businesses couldn't reopen their doors under proper healthguidelines during the coronavirus pandemic.
"I think these businesses need to be open," Cain, from Deer Park, told Fox 26 while getting his haircut.
The news, made during a press conference at the Texas Capitol, added on to an announcement the governor made last week that allowed businesses such as movie theaters and malls to reopen under certain restrictions. And it alleviated pressure that Abbott had been fielding in recent days from mainly Republicans, who argued their constituents needed the businesses they either worked at or owned to reopen because their livelihoods depended on it.
"When you're Greg Abbott and you have people screaming in your ear, you have to find a creative way to communicate with him; he's going 24/7 right now," Toth told the Tribune on Tuesday evening. "We wanted to get a message to the governor — everyone has to take a different tack trying to make sure the governor knows what our constituents are thinking."
Hailey Lankford, a stylist at Tune Up: The Manly Salon in Montgomery County, where Toth and Cain got haircuts, said before Abbott's announcement Tuesday that it’s “essential” for her to go back to work.
“If I do not go back to work, my car will be [repossessed], I will be evicted, I have no choice,” Lankford told the Tribune. “I’m not getting the money from the government along with a lot of other hairdressers I know.”
The salon reopened over the weekend but was quickly shut down by local law enforcement officers who threatened to arrest Lankford and her colleagues if they didn’t close, Lankford said. She added that Tuesday was the salon's first day reopening since that visit from law enforcement. Toth said Tuesday that about three other customers were in the salon while he and Cain were receiving their haircuts.
Cain, for his part, said he was aiming to set an example for constituents — and that his decision to go to the salon Tuesday was simply him carrying out what he has been saying on social media in recent days.
"For me, it was an act of civil disobedience, but it wasn't personal," Cain told the Tribune later Tuesday. "If you've been following my Twitter feed, I was encouraging people to do this — if I was going to encourage others, I should do it myself — to encourage customers to go to any business, whether it's been deemed 'essential' or not, so we can help provide these business owners and employees an income so they can pay their bills."
To be clear, the Houston-area salon was not the only nonessential business going against official orders that shut down many businesses. The city of Dallas is suing the owner of Salon a la Mode for reopening despite local stay-at-home orders. On Tuesday, salon owner Shelley Luther was sentenced to a week in jail for violating a court order to close.
Democrats, meanwhile, argued after Abbott's announcement Tuesday that he was acting prematurely — and that moving to open more businesses in such short order could put Texans at risk.
“From Donald Trump to Greg Abbott to Briscoe Cain and Steve Toth, Texas Republicans have mismanaged and downplayed the seriousness of the coronavirus crisis. It’s time for sensible leadership that keeps the public safe," said Abhi Rahman, a spokesman for the Texas Democratic Party.
Cain, who has also grown a mustache during the pandemic, said he is ready for life to return to some version of normal so that his wife can shave it off.
"I fully realize it's disgusting and needs to go," he said Tuesday evening, "but my mustache is part of me being in mourning for the loss of our civil liberties."
President Donald Trump has handed off another life-or-death matter to his son-in-law and White House senior adviser Jared Kushner.
The president wants a coronavirus vaccine by the end of the year, and he has tasked Kushner to lead those efforts to end the COVID-19 pandemic that's already claimed more than 72,000 American lives, reported The Daily Beast.
“Jared has been vocal in meetings about wanting to engage the private sector on the development of a vaccine in a similarly successful way that the administration did on ventilators, PPE and others,” a White House official told the website.
“President Trump made it clear to the task force weeks ago that business as usual wasn’t good enough in the fight against the coronavirus, and vaccines are no exception” said Michael Caputo, the new assistant secretary of public affairs at the Department of Health and Human Services. “It’s not impossible and yet the scientists are right: it’s going to be very difficult... When it happens, it will be an historic victory for all of America, led by a president who just wouldn’t take no for an answer when it mattered most. Come to think of it, maybe that’s what President Trump’s critics really dislike about it.”
The president is confident a vaccine will be available well before the 12-month timeline researchers cite as a best-case scenario, and Kushner is leading "Operation Warp Speed" with economic adviser Peter Navarro, who pitched the initiative by memo to the coronavirus task force that may soon wind down.
“We were all surprised that [Navarro] was pushing this idea so early on before we knew what supplies we had and where we needed to look to help fill the gaps,” said one administration official. “It was clearly a way to push back against China and a lot of us were uncomfortable doing that in a big way without understanding what we still needed in the stockpiles and elsewhere.”
White House officials hope the president's son-in-law will use his relationships with the private sector to speed up the lengthy development process, two sources told The Daily Beast.
However, not everyone in the White House shares in the president's optimism.
“We just do not see it happening,” said one senior Trump administration official who works closely with the task force.
Navarro claims the development process could be fast-tracked if the medical community operated in "Trump time," but five administration officials who work closely with the task force say that they've seen no evidence that a vaccine could be ready for the general public as soon as the president has promised.
Some of those officials say they have told Trump that his timeline is unrealistic, but he doesn't seem to understand.
When presented with those concerns, those officials said, the president answers some variation of: “I want it done, or I want it taken care of.”