"It projects that if officials move too quickly and too aggressively to reopen in mid-May, individual counties could witness hundreds, if not a thousand-plus, more coronavirus cases reported each day by August 1," said the Beast. "A mere two weeks more of social distancing, the study projects, could result in substantial progress in keeping infections down—with potentially hundreds of thousands of fewer cases if the projections are conservatively expanded out to all 3,000-plus counties across the country."
It is unclear if the White House is preparing for a worsening economy and market in the event that COVID-19 cases grow astronomically and crash the U.S. healthcare system.
In the case of Georgia, Gov. Brian Kemp (R) pushed on with reopening despite continued outbreaks. Now one county in northeastern Georgia is under such strain it is overwhelming their healthcare system. To make matters worse, the grand reopening didn't garner any participants. Malls are still empty. Restaurants are largely empty. Georgia residents aren't stupid - and it's clear they're not willing to put their lives in danger.
According to the models from the PolicyLab, the counties in parts of the country that are expected to have huge outbreaks are both rural and urban. In nearly all cases, they would see significantly lower cases per day if they remained closed until June 1, the projections show. It also shows those continuing to reopen should let counties craft their own laws regulations to let local governments who are more informed about the specifics of their communities make decisions about those areas.
"There's going to be transmission if people stop sheltering in place," said Dr. Rubin, the director of PolicyLab. "It's not that all [counties] are safe to reopen. Every area is extremely sensitive to the amount of distancing you're doing. The more cautious you are, the better."
Critically ill children have been ending up in intensive care units with shock-like symptoms in recent weeks, adding yet another mysterious layer to the coronavirus pandemic.
New York health officials issued an alert on May 4, describing 15 of these cases in New York City. The young patients, ages 2 to 15, had inflammation in multiple organ systems and were described as having features of Kawasaki disease, a rare childhood illness of unclear origin.
A few days earlier, officials in the United Kingdom notified doctors of similar cases there, also describing them as having features similar to Kawasaki disease and toxic shock syndrome. Several of the children had tested positive for COVID-19.
Drawing connections to Kawasaki disease, however, may be premature. Although there are some similarities between the illnesses, there are also many differences.
My clinical practice is as a pediatric infectious disease physician. I also do biomedical research using the body’s immune responses, particularly the antibodies produced, to help find the cause of illness and to help design vaccines. Our group has been collecting samples from Kawasaki disease cases for years. With the COVID-19 pandemic, we responded to the call for researchers and began developing tests to assess the antibody response during COVID-19.
When we started on this path, I did not think these interests would overlap so directly. However, with recent reports of certain COVID-19 cases looking like Kawasaki disease, we are now running tests to see if there is a similar immune response between COVID-19 and Kawasaki disease cases.
Kawasaki versus the new illnesses
Kawasaki disease is an inflammatory condition in children who develop a prolonged fever, inflammation of the mouth and lips, rash, swelling of the hands and feet, inflamed eyes, and lymph node swelling that typically is only on one side of the neck. There can also be incomplete cases that do not have all these symptoms.
Kawasaki disease can have serious consequences: Roughly one-quarter of children diagnosed with it will have inflammation in the vessels that feed the heart, and rarely children will present with heart attacks or shock and need prolonged intensive care.
Unfortunately, we don’t know what causes Kawasaki disease. A litany of viruses, bacteria, fungi and environmental factors have been proposed in the past, including other members of the coronavirus family. Despite not knowing what causes Kawasaki disease, we have found that timely treatments with pooled human antibody preparations – intravenous immunoglobulin, or IVIG – can significantly reduce the heart vessel inflammation.
For the new COVID-19-associated cases showing a significant inflammatory response, many of the reports reflected inthe media and public health announcements have not been published in medical journals. Instead, details have been shared among the medical community in conference calls, message boards and online meetings.
Only one case I know of describing Kawasaki disease associated with COVID-19 has been published. This case, like many of the cases being discussed informally, had no cardiac vessel involvement and lacked a number of clinical symptoms of classic Kawasaki disease.
Some overlap, but different symptoms
There are a number of reasons why the new COVID-19-associated inflammatory disorder and Kawasaki disease seem to be different entities.
Although there is some overlap, these COVID-19-associated cases have fairly different laboratory results. There also tends to be more severe abdominal pain, nausea and vomiting in new cases than would be usual for Kawasaki disease.
The impact on the patient’s heart is focused more on the vessels in Kawasaki disease. The COVID-19-associated cases, in comparison, are globally dysfunctional with only a few describing any vessel inflammation.
The ages and locations of the described new cases are also not typical for Kawasaki disease. Many of the children with severe COVID-19-associated shock are outside the typical age range for Kawasaki disease, which primarily targets children under 7.
The annual case count of Kawasaki disease is also much higher in Asian countries, particularly in Japan, where it is roughly 10 times the rate in North America. I would have expected an association to be described during the first reports of the pandemic, but informal reports from Japan and China don’t appear to describe this severe inflammation in children.
Reports about these new pediatric COVID-19-associated cases are very preliminary. We will learn more as research and details about ongoing and future cases are compiled by the medical community and published for more complete review.
Perhaps studying these new cases will shed much needed light on the cause of Kawasaki disease, a disorder that has perplexed pediatricians for a half-century. As both conditions appear to incite a large inflammatory response in certain children, continued research is needed to provide the “how” for the new COVID-19-associated cases and the “what causes it” for Kawasaki disease.
States such as New York are making the right move by formally gathering data on severely inflamed children during this pandemic, as proper treatments for these new COVID-19-associated cases need to be found.
Coronavirus patients declared recovered who later test positive for the disease are still expelling dead lung cells rather than getting a new infection, the World Health Organization (WHO) told AFP on Wednesday.
South Korean health officials reported more than 100 such cases in April, raising concerns that patients who had recovered could become reinfected.
"We are aware that some patients test positive after they clinically recover," a WHO spokesperson told AFP, without making specific reference to the South Korean cases.
"From what we currently know -- and this is based on very recent data -- it seems they these patients are expelling left over materials from their lungs, as part of the recovery phase."
People infected with the new coronavirus build up antibodies starting a week or so after infection or the onset of symptoms, research has shown.
But it is still not clear, experts say, whether the body systematically builds up enough immunity to ward off a new attack by the virus or, if it does, how long such immunity lasts.
As for the recovered patients who tested negative and then, weeks later, positive, more research is needed, according to the WHO.
"We need systematic collection of samples from recovered patients to better understand how long they shed live virus," the spokesperson said.
"We also need to understand if this means they can pass the virus to other people -- having live virus does not necessarily mean it can be passed to another person."
In a recent interview with BBC, infectious disease epidemiologist Maria Van Kerhove, part of the WHO's Health Emergencies Program, explained the "dead cell" scenario.
"As the lungs heal, there are parts of the lung that are dead cells that are coming up. These are fragments of the lungs that are actually testing positive," she said.
"It is not infectious virus, it's not reactivation. It is actually part of the healing process."
"Does that mean they have immunity? Does that mean they have a strong protection against reinfection? We don't know the answer to that yet."
For some viruses, such as the measles, those who contract it are immune for life.
For other coronaviruses such as SARS, immunity lasted from a few months to a couple of years.
The pandemic has now killed more than 257,000 people globally and officially infected nearly 3.7 million, although with only the most serious cases being tested the number is believed to be far higher.
Critically ill children have been ending up in intensive care units with shock-like symptoms in recent weeks, adding yet another mysterious layer to the coronavirus pandemic.
New York health officials issued an alert on May 4, describing 15 of these cases in New York City. The young patients, ages 2 to 15, had inflammation in multiple organ systems and were described as having features of Kawasaki disease, a rare childhood illness of unclear origin.
A few days earlier, officials in the United Kingdom notified doctors of similar cases there, also describing them as having features similar to Kawasaki disease and toxic shock syndrome. Several of the children had tested positive for COVID-19.
Drawing connections to Kawasaki disease, however, may be premature. Although there are some similarities between the illnesses, there are also many differences.
My clinical practice is as a pediatric infectious disease physician. I also do biomedical research using the body’s immune responses, particularly the antibodies produced, to help find the cause of illness and to help design vaccines. Our group has been collecting samples from Kawasaki disease cases for years. With the COVID-19 pandemic, we responded to the call for researchers and began developing tests to assess the antibody response during COVID-19.
When we started on this path, I did not think these interests would overlap so directly. However, with recent reports of certain COVID-19 cases looking like Kawasaki disease, we are now running tests to see if there is a similar immune response between COVID-19 and Kawasaki disease cases.
Kawasaki versus the new illnesses
Kawasaki disease is an inflammatory condition in children who develop a prolonged fever, inflammation of the mouth and lips, rash, swelling of the hands and feet, inflamed eyes, and lymph node swelling that typically is only on one side of the neck. There can also be incomplete cases that do not have all these symptoms.
Kawasaki disease can have serious consequences: Roughly one-quarter of children diagnosed with it will have inflammation in the vessels that feed the heart, and rarely children will present with heart attacks or shock and need prolonged intensive care.
Unfortunately, we don’t know what causes Kawasaki disease. A litany of viruses, bacteria, fungi and environmental factors have been proposed in the past, including other members of the coronavirus family. Despite not knowing what causes Kawasaki disease, we have found that timely treatments with pooled human antibody preparations – intravenous immunoglobulin, or IVIG – can significantly reduce the heart vessel inflammation.
For the new COVID-19-associated cases showing a significant inflammatory response, many of the reports reflected inthe media and public health announcements have not been published in medical journals. Instead, details have been shared among the medical community in conference calls, message boards and online meetings.
Only one case I know of describing Kawasaki disease associated with COVID-19 has been published. This case, like many of the cases being discussed informally, had no cardiac vessel involvement and lacked a number of clinical symptoms of classic Kawasaki disease.
Some overlap, but different symptoms
There are a number of reasons why the new COVID-19-associated inflammatory disorder and Kawasaki disease seem to be different entities.
Although there is some overlap, these COVID-19-associated cases have fairly different laboratory results. There also tends to be more severe abdominal pain, nausea and vomiting in new cases than would be usual for Kawasaki disease.
The impact on the patient’s heart is focused more on the vessels in Kawasaki disease. The COVID-19-associated cases, in comparison, are globally dysfunctional with only a few describing any vessel inflammation.
The ages and locations of the described new cases are also not typical for Kawasaki disease. Many of the children with severe COVID-19-associated shock are outside the typical age range for Kawasaki disease, which primarily targets children under 7.
The annual case count of Kawasaki disease is also much higher in Asian countries, particularly in Japan, where it is roughly 10 times the rate in North America. I would have expected an association to be described during the first reports of the pandemic, but informal reports from Japan and China don’t appear to describe this severe inflammation in children.
Reports about these new pediatric COVID-19-associated cases are very preliminary. We will learn more as research and details about ongoing and future cases are compiled by the medical community and published for more complete review.
Perhaps studying these new cases will shed much needed light on the cause of Kawasaki disease, a disorder that has perplexed pediatricians for a half-century. As both conditions appear to incite a large inflammatory response in certain children, continued research is needed to provide the “how” for the new COVID-19-associated cases and the “what causes it” for Kawasaki disease.
States such as New York are making the right move by formally gathering data on severely inflamed children during this pandemic, as proper treatments for these new COVID-19-associated cases need to be found.
Why are some people barely affected by coronavirus, while others become gravely ill even though they are young and healthy?
Scientists are searching for answers in patients' genes, looking for mutations that affect their immune response in the hope of finding new treatments.
As more people become infected with the virus, a rough profile of a severely-affected patient has emerged: older, with underlying illnesses and more likely to be male.
But that is far from the full picture.
Intensive care units around the world have also treated a minority of people who are under 50 with no underlying medical problems.
These roughly five percent of patients are the ones that interest geneticist Jean-Laurent Casanova.
"Someone who could have run the marathon in October 2019 and yet in April 2020 is in intensive care, intubated and ventilated," he told AFP.
Casanova, director of the human genetics of infectious diseases laboratory jointly based at the Imagine Institute in Paris and Rockefeller University in New York, wants to find out if they have rare genetic mutations.
"The assumption is that these patients have genetic variations that are silent until the virus is encountered," he said.
Casanova co-founded the COVID Human Genetics Effort, which is seeking to study the genome of these severely-ill younger patients in places like China, Iran, Europe, North America and Japan.
The group is also looking at people who do not become infected despite repeated exposure.
Their research is among a huge global effort involving dozens of labs scouring the genomes of COVID-19 patients for variations that might explain why some people get sicker than others -- and potentially help develop anti-viral therapies.
- Not just 'bad luck' -
Gene mutations have been found to make people more vulnerable to a range of infectious diseases, from influenza to viral encephalitis.
They can sometimes also offer protection.
In the mid 1990s researchers discovered that certain rare mutations of a single gene (CCR5) effectively stopped people from becoming infected with HIV.
The discovery gave researchers a greater understanding of the way the virus worked and paved the way for the development of new treatments.
In the past, whether a person became seriously ill with a particular disease was often put down to "bad luck", said Jacques Fellay, a professor of human genomics of infectious diseases at the Federal Polytechnic of Lausanne.
"Today, we have the capacity to go and dissect the genome of these people and see if they have a rare mutation which could make them particularly susceptible" to the new coronavirus, he told AFP.
But differences in immune response are often caused by multiple genetic factors, Fellay said, likening the body's defence mechanism to a mechanical watch.
"There can be a grain of sand in the cogs. Among a group of patients, each of these grains of sand can be different, but produce the same result", he said.
- Treatment hope -
This complexity means "we need to have a very large sample and collaboration, and the ability to repeat the observation to be confident about the results," said Mark Daly, director of the Institute for Molecular Medicine Finland.
Daly is one of the scientists behind the COVID-19 Host Genetics Initiative, a large-scale global collaboration involving some 150 research centres.
The project aims to recruit at least 10,000 patients and share findings.
Researchers hope to have "very useful information" by the summer, he said, although the timeline is by no means guaranteed.
Ideally the work would lead to treatments.
"There are a huge number of medicines available that target specific genes," Daly told AFP.
"If we find a genetic clue that points us to a gene that already has a medication developed, then we could simply repurpose the drug."
But the process could be much more complicated.
Researchers may find mutations in genes that have not had drugs developed for them -- potentially lengthening the time to create a treatment, said Fellay.
Or worse, they may find that the mutations are not "actionable", or that interventions would create too many side effects.
Discovering the genetic mutations behind immune responses to COVID-19, then, is only the beginning.
"Genetics is a tool for exploring biology, but the resulting treatment, there is nothing genetic about it," he said.
Health officials in Walla Walla, Washington revealed this week that residents are holding "COVID-19 parties" in an effort to spread infections.
"Walla Walla County health officials are receiving reports of COVID-19 parties occurring in our community, where noninfected people mingle with an infected person in an effort to catch the virus," the Walla Walla Department of Health said in a statement on Tuesday.
"While some people with COVID-19 are considered to have mild symptoms, others are at higher risk for severe illness," the statement noted. "Health officials stress that there is much we don’t know about COVID-19. Epidemiologist don’t know if immunity is a sure thing, if reinfection is possible, or if virus could continue living inside you. They do know that even the young can be hospitalized, survivors may suffer long-term damage, and even a ‘mild’ case isn’t mild."
Meghan DeBolt from Department of Community Health told KEPR that coronavirus parties "are not part of the solution."
"They are taking it in the opposite direction because that will lead to an outbreak and every outbreak that we have sets us further away from reopening important social areas of the economy," she explained.
Editor’s Note: As researchers try to find treatments and create a vaccine for COVID-19, doctors and others on the front lines continue to find perplexing symptoms. And the disease itself has unpredictable effects on various people. Dr. William Petri, a professor of medicine at the University of Virginia Medical School, answers questions about these confusing findings.
Some evidence suggests that patients experience low oxygen saturation days before they appear in the ER. If so, is there a way to treat patients earlier?
Even before symptoms arise, people infected with SARS-CoV-2 show damage to their lungs. This is likely why low oxygen saturation – that is, below-normal oxygen levels in their blood – occurs before the patient goes to the ER. Restoring those levels to normal is presumed, though not proven, to be beneficial; giving patients supplemental oxygen via a nasal cannula, a flexible tube that delivers oxygen, placed just inside the nostrils, will restore oxygen to normal levels unless disease worsens to the extent that mechanical ventilation is needed.
Young adults are having strokes with COVID-19. Does this suggest the illness is more of a vascular disease than a lung disease in that age group?
COVID-19 can be a devastating disease to multiple organs and systems in the body, including the vascular and immune systems. A lung infection is the primary cause of disease and death. There are examples of the clotting system being activated and causing strokes, perhaps caused by an immune system responding abnormally to COVID-19.
A sign in a clothing store in Stuart, Florida warns shoppers to keep their distance. Retail stores, restaurants and beaches have now reopened in a majority of Florida counties.
The Centers for Disease Control and Prevention recently updated its official list of symptoms. Does this suggest anything unusual about COVID-19?
This new information is due to a greater number of infected individuals being studied. The update simply reflects a better understanding of the full spectrum of illness due to COVID-19, from asymptomatic to presymptomatic to severe and fatal
infections.
How can so many people experience such mild symptoms and others quickly die from it?
One of the most fascinating aspects of these diseases is the huge difference that individuals experience with an infection. In our own research, we have found that many children in the U.S. infected with cryptosporidia have no symptoms, yet this parasite is a major killer of infants in the developing world. After an infection of SARS-CoV-2, the severity of the illness is likely due in part to how the patient’s immune system responds; an overzealous immune response may cause death through what is called colloquially a “cytokine storm..” We do not know yet if cytokine storms occur more in one group than another – for example, older versus younger.
Thousands of white markers on the grounds of the First Congregational Church in Greenwich, Connecticut. Each marker honors lives lost to the COVID-19 pandemic.
The disease appears now to affect various other organs – heart and kidney, for example. What does this suggest?
What we know most clearly is that infection starts only in human cells with the ACE2 receptor – that is, in a cell that is capable of receiving the virus. That is present not only in the lungs, but in other cells as well, including those in the intestine and in the nasal mucosa, which lines the nasal cavity. When those cells are infected, the immune system is activated. A consequence is that both the heart and kidney are affected.
Why are some countries not experiencing as much COVID-19 as the U.S., Europe and China?
I think it’s too early in the pandemic to know if certain countries or populations are relatively less susceptible. The younger overall age of a population could be a primary factor. Or perhaps the virus, so far at least, has not had time to spread more widely in these countries.
With the FDA approving Gilead’s Remdesivir as an emergency use treatment for the most acute cases of COVID-19, many people are wondering what type of a drug it is.
Remdesivir is a member of one of the oldest and most important classes of drugs – known as nucleoside analogue. Currently there are more than 30 of these types of drugs that have been approved for use in treating viruses, cancers, parasites, as well as bacterial and fungal infections, with many more currently in clinical and preclinical trials.
I am a medicinal chemist who has worked in design and synthesis of these important drug treatments for over 30 years. I have written numerous reviews over the years about these drugs and their structure and function, and as a result have had many inquiries lately from friends, family and others not in the field asking me to explain what exactly is it about Remdesivir that makes it so effective, but also why it is so interesting. Understanding why means digging into the biochemistry of this class of drugs.
Fake genetic building blocks
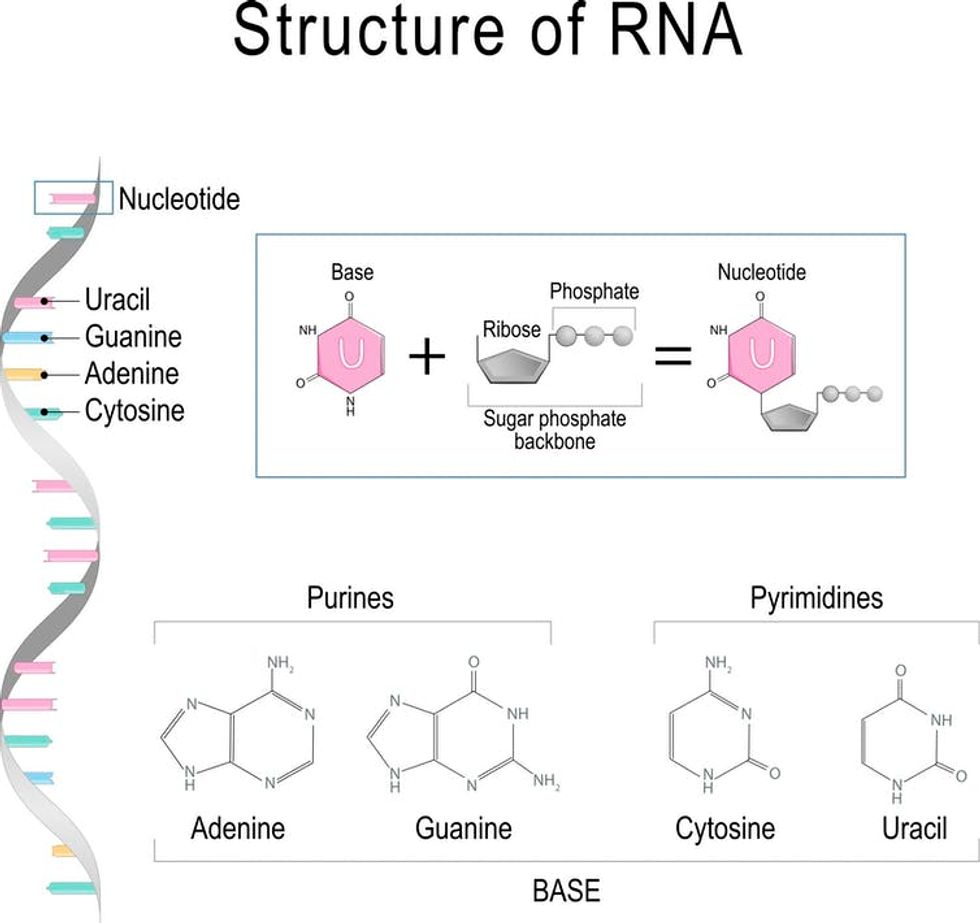
The reason nucleoside analogues and a similar group called nucleotide analogues are so effective is that they resemble the naturally occurring molecules known as nucleosides – cytidine, thymidine, uridine, guanosine and adenosine. These are the essential building blocks for the DNA and RNA that carry our genetic information and play critical roles in our body’s biological processes.
Slight differences in the chemical structure of these analogues from naturally occurring compounds make them effective as drugs. If an organism like a virus incorporates a nucleoside analogue into its genetic material, rather than the real thing, even small changes to the structure of these building blocks prevent the regular chemistry from happening and ultimately foils the ability of the virus to replicate.
The basic structure of a nucleoside includes a sugar group and a base (A, C, G, T or U), and in the case of a nucleotide, a group containing a phosphate which is a collection of oxygen and phosphorus atoms.
Every building block of DNA is made from three parts: a sugar, a base (A, C, G, or T) and a phosphate group. Every building block of RNA is made from (A, C, G, or U).
ttsz / Getty Images
The first nucleoside analogues were approved for medicinal use in the 1950s. The early nucleosides had only simple modifications, typically either to the sugar or the base, while today’s nucleosides, such as Remdesivir, typically have several modifications to their structure. These modifications are essential to their therapeutic activity.
How does Remdesivir work as antiviral therapeutic?
This activity occurs because nucleoside/tide analogues mimic the structure of a natural nucleoside or nucleotide such that they are recognized by, for example, viruses. Due to those structural modifications, however, they stop or interrupt viral replication, which stops the virus from multiplying and infecting more cells in the body.
As a result, they are known as direct-acting antivirals, and this is the case for Remdesivir, which works by blocking the coronavirus’s RNA polymerase – one of the key enzymes that this virus needs to replicate its genetic material (RNA) and proliferate in our bodies. Remdesivir works when the enzyme replicating the genetic material for a new generation of viruses accidentally grabs this nucleoside analogue rather than the natural molecule and incorporates it into the growing RNA strand. Doing this essentially blocks the rest of the RNA from being replicated; this in turn prevents the virus from multiplying.
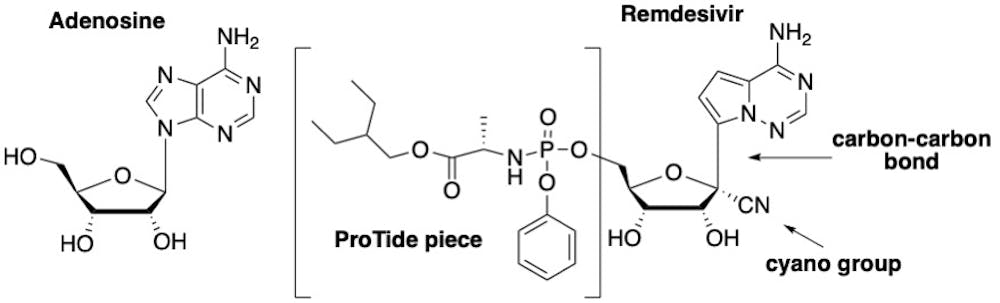
The drug Remdesivir is basically an altered version of the natural building block adenosine – which is essential for DNA and RNA. Comparing the structure of Remdesivir with adenosine, one can see there are three key modifications that make it effective.
The first is that Remdesivir, as it is administered, is not the actual active drug; it is actually a “prodrug,” meaning it must be modified once in the body before it becomes an active drug. Prodrugs are used for many reasons, including protecting a drug until it reaches its site of action. The active form of Remdesivir contains three phosphate groups; it is this form that is recognized by the virus’s RNA polymerase enzyme.
A naturally occurring nucleotide (left) which is a building block of RNA and DNA and Remdesivir (right) which is a variation on its natural counterpart.
The second important modification on Remdesivir is the carbon-nitrogen (CN) group attached to the sugar. Once Remdesivir is incorporated into the RNA growing chain, the presence of this CN group causes the shape of the sugar to pucker, which, in turn, distorts the shape of the RNA strand such that only three more nucleotides can be added. This terminates the production of the RNA strand and is what ultimately sabotages the replication of the virus.
The third important structural feature which makes Remdesivir differ from adenosine is the change of one particular chemical bond on the molecule. Rather than a bond linking a carbon and nitrogen atoms, chemists replaced the nitrogen with another carbon, creating a carbon-carbon bond. This is critical to the success of this drug because coronaviruses have a special enzyme that recognizes unnatural nucleosides and clips them out. But by changing this chemical bond, Remdesivir cannot be removed by the enzyme, allowing it to stay in the growing chain and block replication.
Remdesivir trials
Remdesivir originally was found during a drug discovery program at Gilead to search for inhibitors of the hepatitis C virus, which is another RNA virus. Although Gilead ultimately selected a different nucleoside analogue for treatment of hepatitis the company tested the drug to see if it was effective against other RNA viruses. Remdesivir exhibited potent activity against Ebola and Middle Eastern respiratory virus, among others.
According to the NIH, patients who received Remdesivir had a faster recovery compared to those who received placebo; 11 days compared with 15 days for those who received the placebo. “Results also suggested a survival benefit, with a mortality rate of 8.0% for the group receiving Remdesivir versus 11.6% for the placebo group,” according to the NIH press release.
While these results are preliminary, there are a plethora of clinical trials underway across the world. Regardless, a certain amount of caution is still needed. As noted by Dr. Anthony Fauci on NBC’s “Today” show, “the antiviral drug Remdesivir is the first step in what we project will be better and better drugs coming along” to treat COVID-19, but cautioned, “This is not the total answer.”
I share this view with many other scientists in the field. No matter what those results ultimately show, Remdesivir will mostly certainly be part of a cocktail of drugs, just as is standard for treating other viruses such as HIV and hepatitis C.
A combination, or cocktail, of drugs will provide a more effective and more complete therapy that blocks the virus from replicating. The other benefit of such a drug cocktail is that it lowers the chance the virus will develop resistance to the therapy. In the meantime, these early results for Remdesivir are proving to be an important source of hope for many of us across the world as we wait for this pandemic to subside.
A cargo capsule that was part of a key test in China's space programme experienced an "anomaly" Wednesday during its return trip, the space authority said.
The cargo capsule was launched Tuesday aboard a new type of carrier rocket along with a prototype spacecraft, and the latter is expected to return to Earth on Friday.
The launch is a major test of China's ambitions to operate a permanent space station and send astronauts to the Moon.
But "an anomaly occurred today during the return" of the cargo capsule, the China Manned Space Agency said in a statement.
"Experts are currently analysing the data," it said without offering details.
The cargo capsule was not designed to transport astronauts, only equipment. The device, developed by China Aerospace Science and Industry Corporation, is an experimental prototype.
The capsule was fitted with an "inflatable" heat shield. This type of structure, also being tested by the American and European space agencies, aims to eventually replace the classic metal heat shields that are heavier and thereby reduces the amount of cargo that can be carried into space.
Tuesday's launch was also the maiden flight of the Long March 5B rocket, considered the most powerful rocket made in China to date. State media said the launch was a "success".
It comes after two previous failures when the Long March 7A malfunctioned in March and the Long March 3B failed to take off in early April.
Beijing has invested heavily in its space programme in recent years as it plays catchup to the United States, the only country to have sent a man to the Moon.
Assembly of the Chinese Tiangong space station, whose name means Heavenly Palace, is expected to begin this year and finish in 2022.
China also became the first nation to land on the far side of the Moon in January 2019, deploying a lunar rover that has driven some 450 metres so far.
Five Republican governors crafted an op-ed in the Washington Post Tuesday, singing their own praises for their COVID-19 response without shutting down their government. The problem, however, is that four out of the five governors are in states that are suffering among the highest per capita coronavirus cases in the country.
Govs. Mark Gordon (R-WY), Pete Ricketts (R-NE), Asa Hutchinson (R-AR), Kim Reynolds (R-IA) and Mike Parson (R-MO) announced in the column that while they have different approaches, all of their states have been "open for business," delivering food and other goods.
"Our collective experience ensures that our contribution toward reopening our nation’s economy is stable, safe and durable. Restarting our economy is not a race to be won but a cooperative effort. Our approach has created a model for success that can be applied throughout the country," the editorial says.
As Huffington Post editor Kate Sheppard pointed out, low coronavirus cases in a state doesn't exactly stand up when one considers the population of the state.
Missouri is the 23rd lowest state in terms of population density, but it's the 24th highest in terms of positive test rates.
Using the data chart from Johns Hopkins University Center for Systems Science and Engineering, these Republican states appear to be worse off than some of the most populated counties in the United States.
Wyoming has 101 confirmed cases per 100,000 residents. Arkansas has 114 confirmed cases per 100,000 residents. Missouri has 140 confirmed cases per 100,000 residents. Iowa has 291 confirmed cases per 100,000 people. Nebraska has 293 confirmed cases per 100,000 residents
To put that in context, Los Angeles County, California has 84 per 100,000 people, meaning LA is doing better than all of the GOP states. Similarly, the blue state of Oregon has just 64 confirmed cases per 100,000 residents. Montana, run by a Democratic governor, has just 43 confirmed cases per 100,000 people, for the lowest rate in the country. Maine is also run by a Democratic governor, and the state has 88 confirmed cases per 100,000 people. Hawaii has just 44 confirmed cases per 100,000. All of the Democratic states issued their own stay-at-home orders.
Politico cited the study from "epidemiologists and clinician-researchers at four universities in conjunction with the nonprofit AIDS research organization amFar and PATH’s Center for Vaccine Innovation and Access," using available data on the contraction and fatalities of the virus.
The study then worked to fill in the 78 percent of missing information about ethnicity in the Center for Disease Control's data.
“In small metro areas as well as rural areas, we're seeing disproportionately higher Covid-19 deaths taking place in primarily black counties,” said lead investigator and epidemiologist Gregorio Millett, V.P. of amFar, The Foundation for AIDS Research.
The study is still going through a review from a medical journal before it is published more broadly, but scientists felt it was urgent to release the findings to help influence policy decisions officials are making in real-time.
"The findings back up trends in states such as Wisconsin and Louisiana, which have seen African-Americans hit harder by the coronavirus compared to white residents," said Politico. "The study also found that the disproportionately black counties ravaged by coronavirus cases and deaths also showed high levels of underlying conditions like heart disease, hypertension, and diabetes."
“We know that being uninsured and crowded living conditions are associated with increases in Covid-19 diagnoses among black Americans,” said Millett.
The early days of the COVID-19 crisis didn't show the virus was hitting African-American communities as much, but on March 19 "we see the shift to greater diagnoses in disproportionately black counties.
Out of the 677 disproportionately Black counties in the United States, 91 percent were in the South, explained Politico.
The inordinate toll on Black communities "calls for interventions like considering emergency enrollment for the Affordable Care Act,” said Dr. Patrick Sullivan, professor of epidemiology at Emory University. “And in the longer term Medicaid expansion in the South.”
"As of April 12, there were 283,750 positive coronavirus cases in disproportionately black counties and 12,748 deaths, according to the study. By comparison, all other counties had 263,640 diagnoses and 8,886 deaths," said Politico.
Trump directed Secretary Ben Carson to use the White House Opportunity and Revitalization Council to find ways to help minority communities hit hard by the virus. It's been over a month and Carson still hasn't announced any action or a plan.
A professor at the University of Michigan Law School says that the COVID-19 pandemic has revealed a "fundamental flaw" in America's education system.
In an op-ed for the Detroit Free Press, Professor Len Niehoff argues that students are not being taught about the importance of evidence in making public health decisions.
"We have failed to teach a subject of critical importance, and as a result have imperiled our health, our economy, and our republic," Niehoff writes. "We teach it in law school. We call it Evidence."
COVID-19 has revealed our societal failure to understand what evidence is and to respect how it works. National and local political leaders have made decisions that ignored the evidence. Members of the general public have proved slow to accept the evidence. Measures adopted to help flatten the curve have been met with virulent protests, despite the evidence that they are working.
COVID-19 has no monopoly here. We’ve done little to address global warming, despite the evidence. We pretend the wild escalation of the national debt has no consequences, despite the evidence. And so on.
"We have become a nation of magical thinkers, making decisions based on what we hope is the case and whom we want to believe," Niehoff laments. "When confronted with opposing evidence, we do not engage with it. We dismiss it and stick a label on it: 'fake,' 'phony,' 'biased,' etc. And then we mistake that label for evidence."
Niehoff goes on to suggest that every high school student be required to take a course in evidence.
"Without such training, we will continue to make decisions based not on what is true but on what we wish were true," he warns. "Things like pandemics don’t care about our preferences. They have a ruthless commitment to reality. We need one, too."
"If we don’t, we will not just repeat the errors of the past," Niehoff concludes. "We will blunder into fresh ones that were avoidable, but that our disregard of truth has made apocalyptic."
"The new strain appeared in February in Europe, migrated quickly to the East Coast of the United States and has been the dominant strain across the world since mid-March, the scientists wrote," the Times said.
The study also said that the new strain could make people more vulnerable after a second infection.
The study hasn't been peer-reviewed, but the scientists posted it online at BioRxiv "to speed up collaborations with scientists working on COVID-19 vaccines or treatments." The research has focused largely on sequencing the genes of earlier strains of the virus. The team worked with scientists at Duke University and the University of Sheffield in England to identify 14 mutations of the coronavirus. They're focusing on a mutation called D614G, which the Times pointed to as "being responsible for the change in the virus' spikes."
“The story is worrying, as we see a mutated form of the virus very rapidly emerging, and over the month of March becoming the dominant pandemic form,” said study leader Bette Korber, who serves as a computational biologist at Los Alamos. “When viruses with this mutation enter a population, they rapidly begin to take over the local epidemic, thus they are more transmissible.”
But some scientists are disputing the findings.
"I think those claims are suspect, to say the least," tweeted Harvard Associate Professor Bill Hanage, who works in the School of Public Health. "Major observation: a specific mutation in the spike protein of the virus has been in a higher fraction of cases as the pandemic has worn on in multiple places. Given the role of the spike protein in [the] entry of the virus to cells this might be reasonable."
"Now for the cold water," Hanage continued. "We need to distinguish between selection, in which a variant becomes more common because it leaves more descendants, and founder effects in which a variant becomes more common because it was fortunate rolling the dice by that, I mean this variant might have been lucky and got introduced to places outside Wuhan and different approaches to social distancing early on."
He explained that it isn't about the virus, as much as it is about the environment in which the virus can be transmitted.
"The paper distinguishes between orange and blue variants (you don’t need to be tracking the exact mutation or character state for you wonderful nerds following) the orange is the old one, the blue is the more recent one," he explained.
But the blue mutation is already in all (or close to all) of the cases of the early outbreak in Northern Italy.
"This might be selection," he continued. "It might well also be chance, the lucky strain that got out of China. Most outbreaks around the world descend from Europe now. Meanwhile, China’s extreme interventions appear to have squashed what remained in China and stemmed the dissemination of the other parts of the early viral diversity ([with] strong caveat that there are far fewer genomes from regions that are not Europe or the US)."
He also noted that there are a lack of genomes from the later stages of the pandemic from China and Asia, making it hard to analyze. He explained that more samples from Iran could be helpful, because the genome there appears to be very close to the original strain.
"Essentially the virus has been mutating, as Xueting Qiu and I said it would in February," he went on. It doesn't exactly mean much, however, because mutations happen when genomes replicate. "The increase in the ‘blue’ variant may well reflect a population bottleneck, in which it happens to be the one that gets into the (relatively inattentive) European population and then spreads like wildfire. That's what I *think* happened."