MSNBC host Stephanie Ruhle asserted on Thursday that presumptive Democratic presidential nominee Joe Biden should form a "shadow government" to compete with President Donald Trump's "daily clown show."
In an interview on MSNBC, President Barack Obama's former deputy chief of staff Jim Messina said that Biden's leadership would be a refreshing change from Trump's "daily clown show press conferences" about the coronavirus pandemic.
"Should Joe Biden be counter programming?" MSNBC host Stephanie Ruhle wondered. "Should he be creating his own shadow government, shadow cabinet, shadow SWAT team and getting up there at a podium every night, saying, 'Here's the crisis we're in, here's what we need to do to address this?'"
Messina pointed out that Biden has a plan for combatting the coronavirus and "if Donald Trump was implementing it right now, we'd all be okay."
Messina, however, did not explicitly endorse the idea of a shadow government.
In an op-ed for The New York Times this Thursday, columnist Jennifer Senior writes that President Trump's strategy for reopening the economy is like "offering to use a condom after you’ve already gotten a woman pregnant."
"Donald J. Trump has taken a rather peculiar view of the new coronavirus: If he can’t see the damage it’s doing, it’s not doing any damage," she writes.
According to Senior, Americans have the assumption that a president will plan, self-moderate and reason. But what Trump is doing is the exact opposite. While Trump's disrespect for norms is a characteristic that helped him surge to the presidency, he has nevertheless been slow to admit that life won't be normal after the outbreak.
"Only under duress did he start to encourage a national program of social distancing," Senior writes. "He persisted in shaking hands at news conferences, even when the rest of us were leaving six-foot wedges between ourselves and our fellow citizens. He says that he, personally, won’t wear a face mask."
Senior noted that humans are somewhat “hard-wired” to ignore dangers that they cannot see, citing Harvard social psychologist Daniel Gilbert.
“The apparatus that sees the world is over 400 million years old. The prefrontal cortex — the part of the brain that comprehends projection models from the C.D.C. — is maybe 2.5 million years old. That’s brand-new, in evolutionary terms. It’s still in beta testing,” Gilbert told her.
But Senior said that Trump’s prefrontal cortex appears to be “entirely offline.”
“His plans to fight this pandemic vary from hour to hour, minute to minute. He has all the focus of a moth.”
Senior admits that it wasn't only Trump who was slow to react to the virus. Even Dr. Anthony Fauci admitted that he rode the New York subway in the pandemic's early days -- "Which makes the early action of some of our governors all the more remarkable," Senior writes.
But with the work of stamping out the coronavirus unfinished, Trump is signaling that he wants to reopen the economy sooner rather than later.
"It’s essential to our economic health, it’s true," writes Senior. "But the president refuses to concede there’s a testing problem, and absent testing, it may be hard to get many people to go back outside. Before, no one wanted to be the only chump to avoid crowds; now many will be reluctant to be the chump who rushes toward them."
Estimated deaths from the coronavirus passed 30,000 Americans this week, but that still hasn't stopped President Donald Trump from boasting about his supposedly strong poll numbers.
On Thursday morning, the president tweeted about a purported poll conducted by right-wing news network OAN that showed he had a 52 percent approval rating in North Carolina. The president also gloated that the same poll also showed him besting former Vice President Joe Biden by seven points in the state.
However, many Twitter users were not in the mood to hear the president talking about his poll numbers at a time when 30,000 Americans died from COVID-19 in the last month, and more than 5 million more people filed unemployment claims in just the last week.
President Donald Trump on Wednesday held a call with top Wall Street executives and bankers to discuss reopening the economy. But according to Politico reporter Ben White, things did not go well.
"The whole thing was a bit of a disaster, the way they announced this on Tuesday," White explained on MSNBC, "read a lot of corporate CEO names that had no idea they were a part of this effort to reopen the economy, didn't give anybody really time to plan to be on these calls. Among the Wall Street executives, a lot of them had earnings yesterday and couldn't be on the call. One JP Morgan executive tried for 20 minutes to get in and couldn't."
"What they're telling the president is, yes, of course we want the economy reopened. We want businesses to start up again," he continued. "But we cannot do that, our employees will not feel safe until the testing regime is much more widespread, until people don't feel like they're going out to be guinea pigs to get the virus. There's simply no way to do it that way. Make people feel safe. Make business owners feel like demand is going to be there and then you can start to reopen. So the whole thing was slap dash in the way it was set up, and slap dash in the way it was executed and I think Trump heard a lot of things maybe he didn't want to hear."
According to White's Politico article, one top executive described the call with Trump as a "sh*t show."
President Donald Trump appears hellbent on "reopening" the American economy next month, but American University School of Public Affairs law professor David Malet is warning that it won't be the glorious return to normalcy that the president is craving.
Writing in the Washington Post, Malet says that recent research he's conducted has shown that "much of the public will not tolerate any level of risk -- and will not trust experts or officials who tell them that it’s safe to go out again" during the COVID-19 pandemic.
Citing a study that he conducted last decade, Malet said that many Americans are likely to stay in quarantine during the pandemic even if they're told that they can go out to bars and restaurants again.
"Three months into the exercise, when presented with choices about which quarantine and decontamination approaches to support, virtually every participant opted to try to bring risk down to zero," he writes. "The goal of the study was to determine public tolerance for acceptable risk. The experiment found that no risk levels were acceptable -- even for participants who initially believed there was no risk."
In fact, Malet found that people were so scared of getting infected that they would refuse to come out even when told the risk was absolutely minimal.
"Nearly half the experiment’s total responses involved our ordinary citizens telling us that no actions -- not even the most extreme efforts -- were enough to reassure them," he writes. "One official told us that a 99.99 percent effective treatment for anthrax, which would have required shutting off the city’s water for one week, was unacceptable because 'I don’t want to be the 0.01 percent who gets anthrax.'"
The coronavirus can infect anyone, but recent reporting has shown your socioeconomic status can play a big role, with a combination of job security, access to health care and mobility widening the gap in infection and mortality rates between rich and poor.
Following the 1348 Black Death in Italy, the Italian writer Giovanni Boccaccio wrote a collection of 100 novellas titled, “The Decameron.” These stories, though fictional, give us a window into medieval life during the Black Death – and how some of the same fissures opened up between the rich and the poor. Cultural historians today see “The Decameron” as an invaluable source of information on everyday life in 14th-century Italy.
Boccaccio was born in 1313 as the illegitimate son of a Florentine banker. A product of the middle class, he wrote, in “The Decameron,” stories about merchants and servants. This was unusual for his time, as medieval literature tended to focus on the lives of the nobility.
“The Decameron” begins with a gripping, graphic description of the Black Death, which was so virulent that a person who contracted it would die within four to seven days. Between 1347 and 1351, it killed between 40% and 50% of Europe’s population. Some of Boccaccio’s own family members died.
In this opening section, Boccaccio describes the rich secluding themselves at home, where they enjoy quality wines and provisions, music and other entertainment. The very wealthiest – whom Boccaccio describes as “ruthless” – deserted their neighborhoods altogether, retreating to comfortable estates in the countryside, “as though the plague was meant to harry only those remaining within their city walls.”
Meanwhile, the middle class or poor, forced to stay at home, “caught the plague by the thousand right there in their own neighborhood, day after day” and swiftly passed away. Servants dutifully attended to the sick in wealthy households, often succumbing to the illness themselves. Many, unable to leave Florence and convinced of their imminent death, decided to simply drink and party away their final days in nihilistic reveries, while in rural areas, laborers died “like brute beasts rather than human beings; night and day, with never a doctor to attend them.”
Josse Lieferinxe’s ‘Saint Sebastian Interceding for the Plague Stricken’ (c. 1498).
After the bleak description of the plague, Boccaccio shifts to the 100 stories. They’re narrated by 10 nobles who have fled the pallor of death hanging over Florence to luxuriate in amply stocked country mansions. From there, they tell their tales.
One key issue in “The Decameron” is how wealth and advantage can impair people’s abilities to empathize with the hardships of others. Boccaccio begins the forward with the proverb, “It is inherently human to show pity to those who are afflicted.” Yet in many of the tales he goes on to present characters who are sharply indifferent to the pain of others, blinded by their own drives and ambition.
In one story, a dead man returns from hell every Friday and ritually slaughters a different woman who had rejected him during his lifetime. In another, a widow fends off a leering priest by tricking him into sleeping with her maid. In a third, the narrator praises a character for his undying loyalty to his friend when, in fact, he has profoundly betrayed him over many years.
Humans, Boccaccio seems to be saying, can think of themselves as upstanding and moral – but unawares, they may show indifference to others. We see this in the 10 storytellers themselves: They make a pact to live virtuously in their well-appointed retreats. Yet while they pamper themselves, they indulge in some stories that illustrate brutality, betrayal and exploitation.
Boccaccio wanted to challenge his readers, and make them think about their responsibilities to others. “The Decameron” raises the questions: How should the rich treat the poor during a time of widespread suffering? What is the value of a life?
In our own pandemic – with some of the most well-off now clamoring for the economy to re-open, despite the ongoing spread of the disease – these issues are strikingly relevant.
Martha Phillips knows exactly how it feels to suddenly find oneself up close to — and unprotected from — a deadly virus.In 2014, Phillips, an emergency room nurse, was at the bedside of a suspected Ebola patient in Sierra Leone when the disposable plastic guard protecting her face came loose.“I turned my head quickly and my shield came off,” she recounted. “So I am in an Ebola treatment unit and my eyes are completely exposed.” She stayed calm and quickly left the room.Phillips, 35 at the time, had arrived in a rural corner of northwestern Sierra Leone just as Ebola cases were surging in West ...
Stephen Garcia’s family is frantic. The auto body worker, just 32 years old, has been on a ventilator in a Los Angeles-area hospital for nearly two weeks, gravely ill with COVID-19, unresponsive — and unaware of the battle they’re waging on his behalf.For days, Garcia’s mother, his aunt and his girlfriend have pleaded with doctors at Kaiser Permanente Downey Medical Center to try an experimental treatment — blood plasma from people recovered from COVID-19 — in hopes of saving his life.They know it’s not at all a sure thing. But they’ve seen stories from across the country: an anesthesiologist ...
The number of health care workers who have tested positive for the coronavirus is likely far higher than the reported tally of 9,200, and U.S. officials say they have no comprehensive way to count those who lose their lives trying to save others.The Centers for Disease Control and Prevention released the infection tally Tuesday and said 27 health worker deaths have been recorded, based on a small number of test-result reports.Officials stressed that the count was drawn from just 16% of the nation’s COVID-19 cases, so the true numbers of health care infections and deaths are certainly far highe...
During an interview with MSNBC's "Morning Joe," the former vice president tore Trump to pieces for his almost total lack of empathy for Americans suffering under the twin crises of the pandemic itself and the crippling economic recession that has taken hold in its wake.
"These are people who are frightened and they're looking for leadership" Biden said. "What bothers me, what bothers me so much, is the president of the United States doesn't take responsibility. The president of the United States acts like... nothing is his fault. Nothing is his responsibility. You know, Franklin Roosevelt made the case that, look, just tell the American people the truth... they can handle it. But you have to let them know what you are doing. You have to let them know you understand their pain."
Biden then came back to throttle Trump again for refusing to take any responsibility for the pandemic that is costing the country tens of thousands of lives and millions of jobs.
"The president is supposed to take care of things!" Biden emphasized "He says, 'I take no responsibility for that, it is not my fault, it is somebody else's fault." He is doing the exact -- I know it sounds sort of strange -- but he is doing the exact thing we teach our kids not to do, blame somebody else. Not me, the other guy."
Coronavirus testing in the United States is moving into a new phase as scientists begin looking into people’s blood for signs they’ve been infected by SARS-CoV-2, the virus that causes COVID-19. This technique is called serological testing.
Virologist Daniel Stadlbauer helped develop a serological test to detect SARS-CoV-2 antibodies and helped transfer it from the research lab to the clinical setting. Epidemiologist Aubree Gordon regularly uses serological assays in her research studies on influenza and dengue fever. She’s now established serological testing for SARS-CoV-2 in her research lab.
Here, the collaborators explain how the technology works.
What do these tests look for?
Serological tests for SARS-CoV-2 are blood tests. They look at serum or plasma – basically blood that has been processed to remove the cells – for evidence that at some point you’ve been infected with the coronavirus.
These tests look for antibodies that your body’s immune system generated to fight the infection. So, the tests detect the response to the virus, not the virus itself. They cannot be used early in infection, before a patient’s body has mounted an antibody response.
A serological test may focus on different types of antibodies. It can measure what are called neutralizing antibodies, which protect against the virus in question. Or it may measure what are called binding antibodies, a type that recognizes SARS-CoV-2 but does not necessarily protect against it.
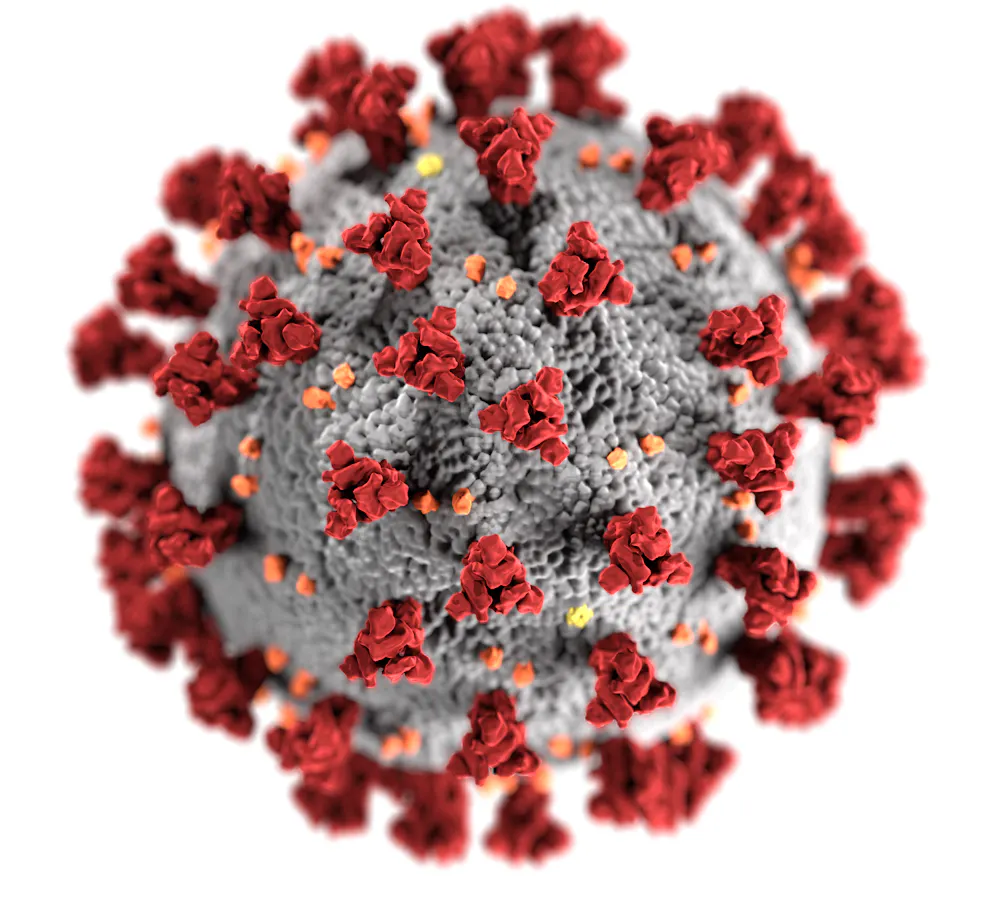
An illustration of one SARS-CoV-2 virus particle shows its spike proteins (in red) scattered across its surface.
Several types of serological tests for SARS-CoV-2 exist. Clinical laboratories and research laboratories typically use what’s called an enzyme-linked immunosorbent assay (ELISA) that consists of plastic plates that are coated with lab-made proteins that match those on the surface of the virus. For the test to be specific, it uses the spike protein from the surface of SARS-CoV-2 that gives the coronavirus its crown-like appearance.
This spike protein is immunogenic, meaning it’s one of the main targets of the body’s immune response; an infected person would make antibodies against the spike protein. The test measures if and how many serum antibodies in the sample bind to the viral proteins on the plates.
Another type of serological test uses what’s called a lateral flow assay. A variety of medical tests, including at-home pregnancy tests, use this technique. It relies on liquid flowing over a pad treated with chemicals that will interact with the molecule you are testing for. Usually the test will indicate the presence or absence of antibodies through easy-to-read lines. They have the benefit of being relatively simple and rapid, but are generally less sensitive and do not give a measure of the amount of antibody present. The FDA has so far approved one test of this type, from the company Cellex.
Why is it helpful to know who has antibodies against the virus?
From a public health perspective, knowing who has already been exposed to SARS-CoV-2 paints a clearer picture of how widespread the virus is in the local population.
Some people are asymptomatic or only came down with mild symptoms, so they might not be counted in other COVID-19 statistics. Epidemiologists can use the serology results to determine how common those cases are. Serological studies can also help figure out a death rate for COVID-19, by clarifying how many people in total have been sick.
Serosurveys are currently generating this kind of data. They use the serological techniques to test a large number of serum samples from people without a confirmed SARS-CoV-2 infection, coming up with statistics about the group as a whole.
Knowing a true rate of infection allows public health workers to better predict the likely future course of the pandemic in individual locations and figure out what interventions are needed to control an outbreak. That’s because researchers think, although no one’s entirely sure yet, that once you have antibodies to the virus it will confer immunity, meaning you’ll be protected for some period of time.
A nurse has blood drawn to check whether she has antibodies to SARS-CoV-2, and hopefully immunity.
Serological testing could also be used to make strategic staffing decisions about essential workers, including medical personnel – for instance, assigning to the front lines those who are have antibodies and are thus presumably immune. These people would be able to go back to work without the risk of getting sick or infecting others.
Identifying individuals who were already infected and who are now potentially immune could play an important part in when and how social distancing restrictions are lifted. Broad SARS-CoV-2 antibody testing could help control the pandemic until a potent vaccine is available – the real coronavirus “end game.”
Where are these tests being performed so far?
Serological testing is already being used to identify people who can serve as plasma donors.
In a process called plasmapheresis, doctors transfer plasma that contains antibodies to a disease into an ill person. Plasmapheresis has been used for decades to treat a variety of diseases.
In this case, plasma from someone who has recovered from COVID-19 – or was infected with the disease but didn’t develop symptoms and has a high level of antibodies – is transferred into a sick patient, typically someone critically ill. At Mount Sinai hospital in New York City, medical workers have started transferring plasma into patients with the hope of neutralizing the virus and alleviating the disease. In other locations, hospitals have started or are preparing to begin this process as well.
Serological testing is also being used to diagnose individual patients who are suspected SARS-CoV-2 cases, but have not tested positive for the virus using the molecular test that looks for the virus’s genetic material.
Multiple serosurveys are underway, or soon will be, in medical systems and in the general population. For instance, Beaumont Hospital System in Michigan has begun a large serosurvey in their medical staff. The Krammer and Simon research labs at Mount Sinai have started a serosurvey with samples from New York City.
No self-administered finger prick tests have yet been approved by the FDA.
Commercial companies have also developed serological tests, including many rapid tests, that are making their way into the marketplace. Ultimately these may be very useful for letting individuals know their infection status. But the currently available commercial tests haven’t been validated by the FDA or a similar authority to say they work well.
There is such high, unmet demand that for the most part, clinical laboratories are choosing to put together their own serological tests, using publicly available instructions, something which is common in research laboratories, but not done as often in U.S. clinical laboratories. Though it takes more time and effort than purchasing ready-to-go tests, which are hard to come by anyway, it provides the clinical labs access to serological tests that have been proven to work well.
Among the most hard-hit are veterans, who are particularly susceptible to both health and economic threats from the pandemic. These veterans face homelessness, lack of health care, delays in receiving financial support and even death.
I have spent the past four years studying veterans with substance use and mental health disorders who are in the criminal justice system. This work revealed gaps in health care and financial support for veterans, even though they have the best publicly funded benefits in the country.
Here are the eight ways the pandemic threatens veterans:
Age and respiratory illnesses are both risk factors for COVID-19 mortality. As of April 13, 241 patients in Veterans Administration health care facilities had died of COVID-19 and 4,000 have tested positive.
2. Dangerous residential facilities
Veterans needing end-of-life care, those with cognitive disabilities, or those needing substance use treatment often live in crowded VA or state-funded residential facilities.
When a person transitions from active military service to become a veteran, they receive a Certificate of Discharge or Release. This certificate provides information about the circumstances of the discharge or release. It includes characterizations such as “honorable,” “other than honorable,” “bad conduct” or “dishonorable.” These are crucial distinctions, because that status determines whether the Veterans Administration will give them benefits.
Research shows that some veterans with discharges that limit their benefits have PTSD symptoms, military sexual trauma or other behaviors related to military stress. Veterans from Iraq and Afghanistan have disproportionately more of these negative discharges than veterans from other eras, for reasons still unclear.
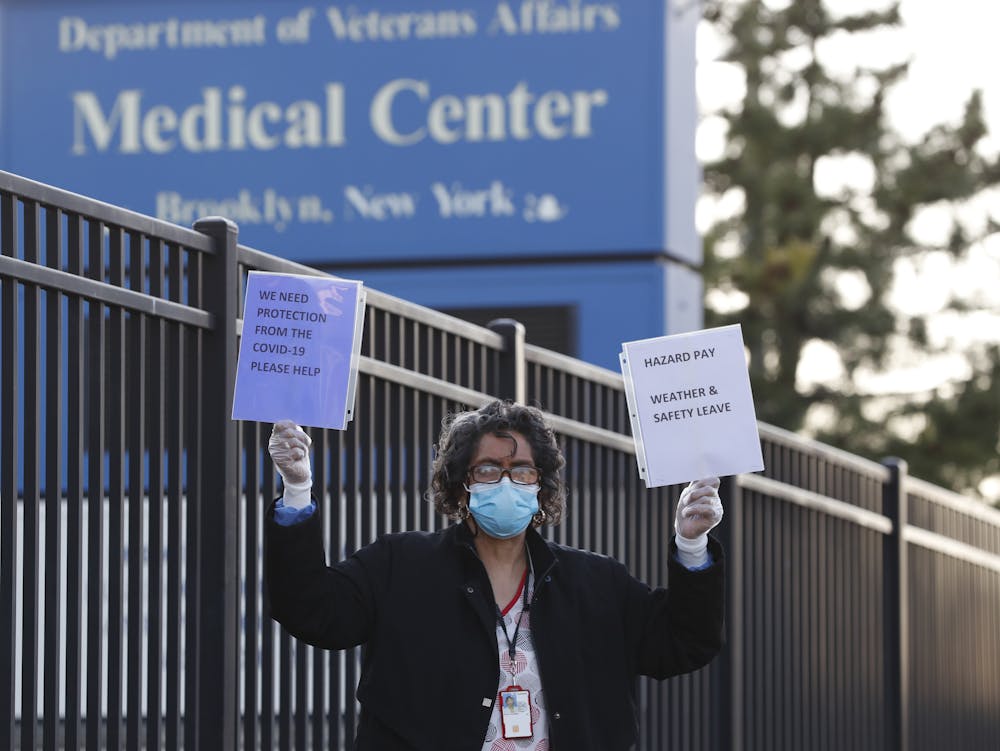
VA hospitals across the country are short-staffed and don’t have the resources they need to protect their workers.
The Veterans Administration frequently and perhaps unlawfully denies benefits to veterans with “other than honorable” discharges.
Many veterans have requested upgrades to their discharge status. There is a significant backlog of these upgrade requests, and the pandemic will add to it, further delaying access to health care and other benefits.
4. Diminished access to health care
Dental surgery, routine visits and elective surgeries at Veterans Administration medical centers have been postponed since mid-March. VA hospitals are understaffed – just before the pandemic, the VA reported 43,000 staff vacancies out of more than 400,000 health care staff. Access to health care will be even more difficult when those medical centers finally reopen.
As of Monday, April 13, 1,520 VA health care workers have tested positive for COVID-19, and thousands of health care workers are under quarantine. The VA is asking doctors and nurses to come out of retirement to help already understaffed hospitals.
5. Mental health may get worse
An average of 20 veterans commit suicide every day. A national task force is currently addressing this scourge.
6. Complications for homeless veterans and those in the justice system
An estimated 45,000 veterans are homeless on any given night, and 181,500 veterans are in prison or jail. Thousands more are under court-supervised substance use and mental health treatment in Veterans Treatment Courts. More than half of veterans involved with the justice system have either mental health problems or substance use disorders.
As residential facilities close to new participants, many veterans eligible to leave prison or jail have nowhere to go. They may stay incarcerated or become homeless.
Courts are moving online or ceasing operations altogether. It is unclear whether participants will face delays graduating from court-supervised treatments.
Further, some Veterans Treatment Courts still require participants to take drug tests. With COVID-19 circulating, participants must put their health at risk to travel to licensed testing facilities.
As veterans’ facilities close to new participants, many veterans eligible to leave prison or jail have nowhere to go and may become homeless, like this Navy veteran in Los Angeles.
In the pandemic’s epicenter in New York, tens of thousands of veterans should have access to VA benefits because of their low income – but don’t, so far.
The pandemic has exacerbated existing delays in finding veterans in need, filing their paperwork and waiting for decisions. Ryan Foley, an attorney in New York’s Legal Assistance Group, a nonprofit legal services organization, noted in a personal communication that these benefits are worth “tens of millions of dollars to veterans and their families” in the midst of a health and economic disaster.
All 56 regional Veterans Administration offices are closed to encourage social distancing. Compensation and disability evaluations, which determine how much money veterans can get, are usually done in person. Now, they must be done electronically, via telehealth services in which the veteran communicates with a health care provider via computer.
But getting telehealth up and running is taking time, adding to the longstanding VA backlog. Currently, approximately 75,000 veterans wait more than 125 days for a decision. (That is what the VA defines as a backlog – anything less than 125 days is not considered a delay on benefit claims.)
8. Obstacles to getting stimulus checks
Veterans with the greatest financial need may not automatically receive their stimulus checks. Currently, those living on tax-exempt income from the VA must file a tax return to get a check.
But e-filing a tax return is a significant obstacle for many, especially severely disabled veterans who may not have computers or know how to use e-file software.
There are many social groups to pay attention to, all with their own problems to face during the pandemic. With veterans, many of the problems they face now existed long before the coronavirus arrived on U.S. shores.
But with the challenges posed by the situation today, veterans who were already lacking adequate benefits and resources are now in deeper trouble, and it will be harder to answer their needs.
More than 2 million coronavirus cases have been reported across the world, affecting 185 countries. But North Korea says it is completely free of the virus, a claim that has been met with scepticism in some quarters. France 24 spoke to Daniel Wertz, program manager at the US-based National Committee on North Korea to find out more.
Pak Myong Su, the director of North Korea’s anti-epidemic headquarters, told AFP earlier this month that "not one single person has been infected with the novel coronavirus in our country so far”.
The claim was disputed by General Robert Abrams, commander of United States Forces Korea, who said it was “impossible” that the secretive authoritarian state did not have a single case of the virus.
“In all likelihood there have been a number of unconfirmed cases,” agreed Wertz, but added that a lack of testing may mean that any outbreak may have gone undetected.
Nevertheless, North Korea’s prompt action in sealing its borders and imposing quarantine measures early on in the coronavirus outbreak could mean that a large outbreak has been avoided, at least for now.
“Back in January, North Korea sealed its borders and began imposing internal quarantines even before the city of Wuhan in China was fully sealed off, which in hindsight looks like it was actually smart for the most part,” said Wertz.
But, he added: “Even if North Korea’s avoided a worst-case scenario, that could change rapidly in the future.”
With poverty and malnutrition rife, coupled with poor healthcare infrastructure, a full-scale coronavirus outbreak in the country could prove devastating, said Wertz.
“Even in the capital a lot of hospitals have to reuse basic medical supplies such as syringes and scalpels. If there was a large coronavirus outbreak in North Korea, I think the country’s public health system would be badly unprepared to deal with it,” he said.











{kind=link}